Weight Control Behaviors among Female University Students in Saudi Arabia
Rawan Alsehli 1, Haya Aljadani 2, 3*
1 BCs, A Research Assistant, Food and Nutrition Department, Faculty of Human Sciences and Design, King Abdulaziz University, Jeddah, Saudi Arabia.
2 Ph.D. in Nutrition and Dietetics from the University of Newcastle, Australia.
3 Assistant Professor, Food and Nutrition Department, Faculty of Human Sciences and Design, King Abdulaziz University, Jeddah, Saudi Arabia.
*Corresponding Author
ABSTRACT
Weight control behaviors (WCBs) are common among university students, however, not all WCBs are healthy and safe. Unhealthy WCB is common among female students especially those who suffer from excess weight. Understanding personal WCBs are important to explore because it is relevant to public health. Therefore, the main aims of the study were to explore WCB followed by female students with BMI ≥ 18.5 kg/m2 at a university located at Jeddah of Saudi Arabia, and to explore what was the main source of information about how to lose or maintain weight. A cross-sectional study was carried out at the female campus of King Abdulaziz University. Information about demographics and history of various healthy and unhealthy WCBs was collected from participants. Weight and height were measured by a trained research assistant and BMI was calculated. A total of 238 students were included in the analysis, more than half of whom (58.8%) followed one or more of WCBs in the last 12 months. 47.9%, 10.9% of the total sample aimed to lose or maintain their current weight, respectively. The majority of overweight and obese (87.3%) students were on attempts to lose weight. Healthy WCB were more common than unhealthy WCB. While out of 5 selected unhealthy WCB, skipped meals (57.9%) and fasting (42.1%) were the most common unhealthy practices. Motivation to follow WCB was to improve appearance (41.4%) and social media was the main source of the information about WCB. Fortunately, it seems that most of the overweight/obese students were aware of their weight and sought weight loss by following healthy WCB, however, the information about WCB obtained from social media may mislead them to imprecise information.
Key words: weight control behaviors, female, weight, obesity, Saudi, social media
INTRODUCTION
Unhealthy dietary choices and sedentary behaviors are major factors contributing to the high incidence of overweight and obesity among Saudi adults. [1-3] Saudi university students tend to have unhealthy eating habits and low levels of physical activity, [4-8] with research showing that they do not meet the daily recommendations for fruit and vegetable intake, often giving preference to discretionary foods and sweet beverages. [4, 5, 9, 10] Unhealthy food habits and insufficient physical activity can lead to increased weight, influencing future health outcomes. [9, 11-16] However, these factors are modifiable through lifestyle and dietary changes [17]. Adopting a healthy lifestyle in early adulthood to prevent obesity-related comorbidity is critical. [18-20]
Female university students are often concerned about their appearance, [21] driving them to engage in unhealthy behaviors to manage their weight. [21-25] Unhealthy weight control behaviors (WCBs) are common among university students, especially those who are dissatisfied with their appearance or carry excess weight. [23, 26] Major examples of unhealthy WCBs include dietary restrictions, fasting, and purging through laxative misuse or vomiting. [22, 27] These behaviors can initially lead to rapid weight loss; however, they increase the risk of future weight regain and the development of mental health disorders. [22, 27] Moreover, unhealthy WCBs do not meet international and national guidelines, which focus on increased physical activity, increased intake of healthy foods, and reduced intake of energy-dense foods. [28-30] In contrast to unhealthy WCBs, healthy behaviors to manage weight include increased physical activity, calorie counting, increased fruit and vegetable intake, and decreased intake of fast foods and foods high in fat and sugar.[11, 27, 30, 31]
In an attempt to manage their weight and improve their appearance and, students may be influenced by peers, family members, and social media, potentially resulting in low-quality information.[13, 32-35] Social media is an online platform that promotes communication, interaction, and content sharing. Weight management and dieting are popular social media topics posted by bloggers as a means of personal promotion, [33] and food is a popular niche marketing topic. Thus, numerous bloggers and organizations attempt to promote their personal dietary practices and weight loss strategies. Social media is not the only influence on behavior. Food industries, especially junk food outlets, those with commercial interests, and other dubious organizations, aggressively promote their services, typically targeting young adults. [36, 37]
Saudi university students often follow unhealthy lifestyle behaviors, and obesity is a common problem; [1] thus, university students, especially females and those with excess weight, may seek rapid results and engage in unhealthy WCBs to control their weight. In addition, research on WCBs in Saudi university students is lacking. Therefore, it is important to identify the behaviors in which students engage, whether these behaviors are healthy or unhealthy, and whether weight affects behavioral choices. Moreover, students’ sources of information about weight loss are unclear; thus, it is important to explore whether sources are professional or social and whether they may potentially mislead students.
Therefore, this study aimed to investigate personal WCBs among female university students with normal or excess weight (overweight or obesity) and the primary sources they use to obtain information. The study is relevant to public health because of increased rates of obesity in the community and its consequences. In addition, it will guide health professionals who work with diet to help those in need of weight loss programs. [38]
mATERIALS AND Methods
This cross-sectional study was conducted on the King Abdulaziz University campus in western Saudi Arabia. Inclusion criteria included non-pregnant female students who were generally healthy (defined as being free of diseases such as type 1 diabetes) and with a body mass index (BMI) of at least 18.5 kg/m2. Individuals with both normal and excess weight were included because the incidence of overweight and obesity is common among university students, and this study focused on exploring personal WCBs in those who wished to lose or maintain their current weight. After being informed about the aims of the study, students who met the inclusion criteria were invited to participate. Those who agreed and provided consent were given a questionnaire in Arabic to complete. The first part of the questionnaire collected participants’ basic demographic information, including age, educational background, marital status, household income, and duration and frequency of physical activity. The second part of the questionnaire collected details about participants’ WCBs (see the following section for more details).
Body Mass Index Measurement
Participants’ weight and height were measured by a research assistant. Weight in kilograms (kg) was measured using a portable scale. Participants were asked to remove their shoes, bags, and coats before being weighed. Each student was weighed twice, with the final weight value being the mean of the two measures. Height in centimeters (cm) was measured using a stadiometer. BMI was calculated from the weight and height values. As mentioned above, only those with a BMI of greater than 18 kg/m2 were included in the study. Participants were classified into two groups: 1) those of normal weight (BMI of 18.5–24.9 kg/m2) and 2) those who were overweight or obese (BMI ≥ 25 kg/m2). [39]
History of Weight Control Behaviors
The second part of the questionnaire comprised of a number of questions on participants’ WCB history. The first question asked students whether they were currently on a diet or engaging in any behaviors to control their weight. Based on their answers, participants were classified into two groups (seekers and non-seekers of weight control). The second question was aimed only at those seeking to control their weight and pertained to their overarching goals. Participants were asked to choose one of the following three goals: 1) to lose weight, 2) to maintain weight, or 3) to gain weight. The next questions asked the seekers of weight control weight whether they had engaged in any of the following WCBs over the previous 12 months: five healthy behaviors—calorie counting, increased physical activity, decreased intake of sweets, decreased intake of fatty foods, and increased consumption of fruit and vegetables—and five unhealthy behaviors—fasting, skipping meals, vomiting, taking laxatives or diuretics to lose weight, and bariatric surgery. Students were also asked whether they had noticed any positive effect on their weight from any of the behaviors. A final question asked them to choose one of the following motivation factors of controlling their weight:1) improved appearance, 2) improved health, 3) improved social life, or 4) be fit.
Statistical Analysis
A descriptive analysis was performed using Stata 14. Frequencies, percentages, means, and Standard Deviations (SD) were used to describe the variables. Pearson’s chi-squared (χ2) and independent t-test were used to test the differences between those seeking and not seeking weight control according to sociodemographic variables. Results were considered significant if p < 0.05.
Table 1: Sociodemographic characteristics of 238 University Students in Saudi Arabia
|
|
Total sample (n=238) |
Seekers of weight control (n=140, (58.8%)) |
Non-seekers of weight control (N=98, (41.2%)) |
P-value |
|
Mean age Mean (SD) |
21.9 (3.4) |
21.9 (3.4) |
21.9 (3.4) |
0.97a |
|
weight (kg) mean (SD) |
58.9(12.3) |
61.3(14.5) |
55.6(7.0) |
0.00b a |
|
BMI (kg/m2) Mean (SD) |
23.8(4.50) |
24.7(5.3) |
22.5(2.7) |
0.00 b a |
|
BMI categories N (%) |
|
|
|
0.00 b |
|
Normal |
136(57.1%) |
51(37.5%) |
85(62.5%) |
|
|
Overweight and obese |
102(42.9%) |
89(87.3%) |
13(12.7%) |
|
|
Household income N (%) |
|
|
|
0.16 |
|
15000 or less |
187(78.6%) |
104(55.6%) |
83(44.4%) |
|
|
More than 15000 |
51(21.4%) |
36(70.6%) |
15(29.4%) |
|
|
Marital Status N (%) |
|
|
|
0.17 |
|
Married |
30(12.6%) |
11(36.7%) |
19(63.3%) |
|
|
Unmarried |
208(87.4%) |
129(62.0%) |
79(38.0%) |
|
|
Education specialty N (%) |
|
|
|
0.42 |
|
Foundation |
12(5.0%) |
9(75.0%) |
3(25.0%) |
|
|
Science |
78(32.8%) |
43(55.1%) |
35(44.9%) |
|
|
Humanities |
148(62.2%) |
88(59.5%) |
60(40.5%) |
|
|
Frequency of physical activity per week N (%) |
|
|
|
0.03 b |
|
Once/ week |
27(11.3%) |
14(51.9%) |
13(48.1%) |
|
|
Twice/ week |
35(14.7%) |
18(51.4%) |
17(48.6%) |
|
|
Three times/week |
45(18.9%) |
27(60.0%) |
18(40.0%) |
|
|
4 times or more/week |
131(55.0%) |
81(61.8%) |
50(38.2%) |
|
|
Time of doing any type of physical activity N (%) |
|
|
|
0.01 b |
|
Below 15 min/day |
45(18.9%) |
22(48.9%) |
23(51.1%) |
|
|
15 to 30 min/day |
121(50.8%) |
80(66.1%) |
41(33.9%) |
|
|
More than 30 min/day |
72(30.3%) |
38(52.8%) |
34(47.2%) |
|
SD: standard deviation, b significant if p-value >0.05, a Independent t-test was conducted while Pearson Chi-square test was conducted for nominal data
Table 2: The Frequency of each of the weight control behaviors for the 140 seekers of weight control
|
|
Seekers of weight control N(%) |
|
Were you currently on a diet or engaging in any behaviors to control your weight? |
140 (100%) |
|
Goals of weight control behaviors |
|
|
loss weight |
113(80.7%) |
|
Gain weight |
4(2.9%) |
|
Maintain weight |
23(16.4%) |
|
Have you engaged in any of the following behaviors to control your current weight? |
|
|
Healthy behaviors |
|
|
Counting calories |
60(42.9%) |
|
Increased physical activity |
103(73.6%) |
|
Decreased intake of sweets |
116(82.9%) |
|
Decreased intake of fatty foods |
103(73.6%) |
|
Increased consumption of fruit and vegetables |
95(67.9%) |
|
Non-healthy behaviors |
|
|
Fasting to control weight |
59(42.1%) |
|
Laxative or Diuretic |
10(7.1%) |
|
Diet pills |
12(8.6%) |
|
Skipping meals |
81(57.9%) |
|
Vomiting |
11(7.9%) |
|
Bariatric surgery |
1(0.7%) |
|
Reason for motivating of WCB |
|
|
Improved appearance |
58(41.4%) |
|
Improved health |
20(14.2%) |
|
Improved social life |
1(0.7%) |
|
Be fit |
14(10.0%) |
|
Missing data |
47(33.6%) |
Results
In total, 238 students met the inclusion criteria and were recruited. The mean (SD) age of participants was 21.9 (3.4) years, and the mean BMI was 23.8 (4.7) kg/m2. At the time of the study, 140 participants (58.8%) were engaged in one or more WCBs to control their weight. The mean (SD) weight of participants engaged in WCBs (61.3 kg (14.5)) was higher significantly than the mean weight of those who were not engaged in WCBs (55.6 kg (7.0)) (p < 0.05). Moreover, most overweight/obese participants were attempting to lose weight (n = 89, 87.3%), while the rest (12.7%) were not attempting to lose weight. With respect to physical activity, participants who were engaged in WCBs were slightly more active in terms of duration and frequency than those who were not engaged in WCBs (p < 0.05) (see Table 1).
Table 2 shows the frequency of each of the WCBs for the 140 participants who were attempting to control their weight. The primary aim of students who were engaged in one or more WCBs was to either lose weight (80.7%) or maintain weight (16.4%), while only 2.9% aimed to gain weight. Students mainly reported healthy practices to control their current weight, including reduced sweet consumption (82.9%), decreased intake of fast foods (73.6%), increased physical activity (73.6%), increased consumption of fruit and vegetables (67.9%), and counting calories (42.9%). A high percentage of students engaged in two of the unhealthy WCBs—skipping meals (57.9%) and fasting (42.1%). However, other unhealthy WCBs were less common: 8.9% of participants used diet pills, 7.9% engaged in vomiting, and 7.1% took laxatives or diuretics. Surprisingly, one student (0.7%) had undergone bariatric surgery. The greatest motivation to control weight was the desire for improved appearance (41.4%).
Figure 1 shows that the most popular source for obtaining information about WCB was social media, followed by books, while professional sources were the least used source of information.
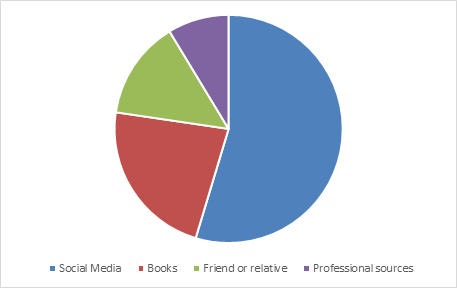
Figure 1: Most popular source for obtaining information about weight control behaviors
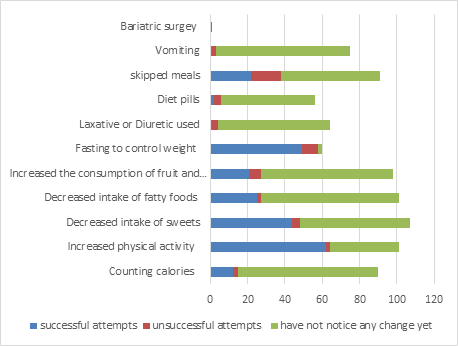
Figure 2: Participants’ most successful attempts to meet their goals based on their experiences
Figure 2 shows participants’ most successful attempts to meet their goals based on their experiences. Many students reported that they had not yet noticed any changes in their weight. Both healthy and unhealthy behaviors were reported as being effective for weight loss, with increased physical activity being the most successful strategy, followed by fasting, eating fewer sweets, skipping meals, and increased consumption of fruit and vegetables.
Discussion
Research on personal WCBs among Saudi university students is limited. It is also unclear whether female Saudi university students who are overweight or obese seek to control their weight more than those with normal weight or the types of WCBs in which they engage. This study aimed at exploring personal WCBs in 238 female Saudi students at a university located in western Saudi Arabia and identifying the main sources used to obtain information about weight control. Participants with normal and excess weight were included in the study.
The results revealed that more than half of the sample (58.8%) followed one or more WCBs. Of the participants engaging in WCBs, the majority (80.7%) were aiming to lose weight, 16.4% were aiming to maintain their current weight, and only 2.9% were aiming to gain weight. These findings align with those of a systematic review, which showed that the majority of weight control seekers aim to lose weight through WCBs, followed by those who aim to maintain their weight. [40]
Regarding participants’ weight, our study revealed that there was a significant difference in weight between those who were seeking weight control and those who were not, with means (SD) of 61.3 (14.5) kg and 55.6 (7.0) kg, respectively. There was also a significant difference in weight status between the two groups (p < 0.05), with most overweight/obese participants (n = 89, 87.3%) attempting to control their weight. Similar to our results, a study found that the higher the BMI of students, the more WBC strategies they used. [41] Another study found that 82.0% of women with moderate or severe weight-related health risks engaged in personal WCBs. [42]
Although most weight control seekers were either overweight or obese, the majority of them engaged in healthy WCBs. We found that 82.9% of weight control seekers ate fewer sweets, 73.6% ate fewer fatty foods, 73.6% increased their physical activity, 67.9% increased consumption of fruit and vegetables, and 42.9% counted calories to control their current weight. These findings contrast with those of other studies that found that overweight and obese people are more likely to engage in unhealthy behaviors. [23, 43]
Two unhealthy WCBs commonly followed by the students in this study were skipping meals (57.9%) and fasting (42.1%). However, other unhealthy WCBs were not common among weight control seekers: only 8.9% took dietary pills, 7.9% practiced vomiting, and 7.1% consumed laxatives or diuretics to control their weight. These unhealthy behaviors are associated with future weight gain and higher levels of psychopathology and psychosocial impairment, [43, 44] warranting further investigation of compensatory behaviors. Notably, people less satisfied with their current weight are more likely to engage in unhealthy WCBs such as fasting, skipping meals, and use of diet pills.[23, 27, 43] Surprisingly, one student (0.7%) had undergone bariatric surgery. This warrants further research attention because females at this stage of life should use measures other than surgery to lose weight. More intervention studies to promote university students’ lifestyle behaviors are urgently needed.
Although the majority of participants seeking to control or lose weight followed healthy behaviors, it was found that the main sources of information for WCBs were poor. Most respondents reported using social media as their main source of information, while a professional source was the least frequently used source. Engaging in social media is common in young adults; however, social media, which is mainly used as a commercial marketing platform, is a poor source of information about healthy behaviors, [33, 37, 45] leading to students believing that skipping meals, fasting, vomiting, and use of diet pills, laxatives, or diuretics are effective means of losing weight. It is recommended that Saudi researchers should focus on the use of social media as a tool to improve young people’s health and weight outcomes and add valuable content about healthy lifestyle behaviors, including healthy WCBs. Professional advice, which is more effective for preventing and managing obesity, should be accessible through public healthcare centers. [38] More research is required in the field to understand the sources of social media information that are the most useful. Further research should consider the implementation of classes or other means of educating students as part of the university community.
From our study, it may be concluded that the majority of students suffering from excess weight were seeking to lose weight, and most of these students were engaged in healthy WCBs, implying that they were aware of the problem and were willing to change their lifestyles. A systematic review has confirmed that university can be a great platform to promote healthy habits and thus prevent future weight gain. [20] Thus, future intervention studies targeting university students are recommended to prevent future health issues in Saudi populations. Although weight control is challenging, it is achievable by following professional recommendations and engaging in healthy behaviors.
The World Health Organization recommends that the key strategy for weight management is to control energy balance by consuming a healthy diet, including limiting energy intake from fats and free sugars and increasing fruit and vegetable consumption, and increasing physical activity. [30] Other studies have shown that dietary strategies are among the most common and successful WCBs. [46, 47] However, the most successful attempts identified from participants’ responses in this research were increased physical activity, followed by a mix of unhealthy and healthy behaviors. In addition, this study found significant differences in the duration and frequency of physical activity between those who did and did not engage in WCBs. However, we did not identify the type, intensity, or amount of physical activity.
Fasting or restricted eating was the second most successful strategy after physical activity. Indeed, increased physical activity is a commonly accepted weight-loss strategy, [48, 49] while fasting or dietary restrictions are only partially accepted in the community as a means of weight loss. [50, 51] Other successful behaviors to control weight reported by students were restricting the consumption of energy-dense food such as sweet and fatty foods, followed by skipping meals. While, decreased intake of foods high in sugar and fat is an effective means of weight management, [30], there is limited research with respect to skipping meals, which in many cases can lead to weight gain, [52]
This study found that an increased intake of fruit and vegetables was another successful way to control weight. A systematic review [53] found that increased fruit and vegetable intake is effective for weight loss among those with excess weight. Unfortunately, Saudi university students have insufficient intake of fruit and vegetables.[4, 6, 54] Thus, it is important to advise this group to increase their consumption of fruit and vegetables for health reasons. A major limitation of this research in terms of the most successful WCBs is that many students had not yet noticed changes and were not followed up.
Given that fasting and skipping meals are two of the most controversial means of weight control, further research on these two behaviors is warranted. Moreover, the role of a healthy diet in weight loss is currently under research. However, existing strategies have previously been shown to be effective. Physical activity is a major and modifiable factor that should be adopted for a healthy lifestyle in general, for not only weight management, but also better health and life quality. One review found that Saudi females are inactive. [7] Thus, it is recommended to implement physical activity promotion programs, especially for those at a greater risk of obesity. Thus, future research should be conducted to ensure that physical activity is implemented as part of university curricula.
The findings of this study are important. A strength of this study is the use of weight and height measures. Limitations include no assessment of family or dietary preferences and a lack of participant follow up. Moreover, participation was voluntary, and the study did not identify the weight students had lost or aimed to lose.
Conclusion
This study showed that most of the sample were following healthy WCB, however, a considerable number of those followed unhealthy behaviors including skipped meals and fasting. In addition, the main source of their information about WCB was social media and so, it is recommended to enhance the role of professionals in this matter.
Acknowledgments
The authors would thank participants for participating in this study.
REFERENCES
- Balhareth A, Meertens R, Kremers S, Sleddens E. Overweight and obesity among adults in the Gulf States: A systematic literature review of correlates of weight, weight-related behaviours, and interventions. Obes Rev. 2019;20(5):763-793.
- Memish ZA, El Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S. Obesity and Associated Factors - Kingdom of Saudi Arabia, 2013. Prev Chronic Dis. 2014;11:E174.
- Mahassni SH. Overweight and Obesity and the Immune System, Lipids and C-reactive Protein in Young and Middle-aged Saudi Female University Workers. J. Biochem. Technol. 2020;11(1):49-56.
- Al-Rethaiaa AS, Fahmy A-EA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutr J. 2010;9(1):39.
- Khalaf A, Westergren A, Berggren V, Ekblom Ö, Al-Hazzaa HM. Prevalence and association of female weight status and dietary habits with sociodemographic factors: a cross-sectional study in Saudi Arabia. Public Health Nutr. 2015;18(5):784-796.
- Al Qauhiz NM. Obesity among Saudi Female University Students: Dietary Habits and Health Behaviors. J Egyp Public Health Assoc. 2010;85(1-2):45-59.
- Al-Hazzaa HM. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci (Qassim). 2018;12(6):50-64.
- Almutairi KM, Alonazi WB, Vinluan JM, et al. Health promoting lifestyle of university students in Saudi Arabia: a cross-sectional assessment. BMC Public Health. 2018;18(1):1093.
- Crovetto M, Valladares M, Espinoza V, et al. Effect of healthy and unhealthy habits on obesity: a multicentric study. Nutrition. 2018;54:7-11.
- Sui Z, Wong WK, Louie JCY, Rangan A. Discretionary food and beverage consumption and its association with demographic characteristics, weight status, and fruit and vegetable intakes in Australian adults. Public Health Nutr. 2017;20(2):274-281.
- Institute of Medicine. Weight Management: State of the Science and Opportunities for Military Programs. Washington, DC: The National Academies Press; 2003.
- Fedewa MV, Das BM, Evans EM, Dishman RK. Change in Weight and Adiposity in College Students: A Systematic Review and Meta-Analysis. Am J Prev Med. 2014;47(5):641-652.
- Hruby A, Hu FB. The Epidemiology of Obesity: A Big Picture. Pharmacoeconomics. 2015;33(7):673-689.
- Chen C, Ye Y, Zhang Y, Pan X-F, Pan A. Weight change across adulthood in relation to all cause and cause specific mortality: prospective cohort study. BMJ. 2019;367:l5584.
- Alshaikh MK, Filippidis FT, Baldove JP, Majeed A, Rawaf S. Women in Saudi Arabia and the Prevalence of Cardiovascular Risk Factors: A Systematic Review. J Environ Public Health. 2016;2016:7479357-7479357.
- Mahassni SH, Munshi MA. Ground Lepidium Sativum Linn Seeds Mixed with The Regular Diet of Rats Lead to Higher Body Weight and Body Weight Gain. Pharmacophores. 2019;10(4):49-56.
- Darkhor S, Estebsari F, Hosseini M, Charati JY, Vasli P. Effect of health promotion intervention on Nurses’ healthy lifestyle and health-promoting behaviors: RCT study. J. Adv. Pharm. Educ. Res. 2018;8(1):108-14.
- Ba S, I C, Jc S, Wpt J. Diet, nutrition and the prevention of excess weight gain and obesity. Public Health Nutr. 2004;7(1a):123-146.
- World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneva2013.
- Plotnikoff R, Collins CE, Williams R, Germov J, Callister R. Effectiveness of Interventions Targeting Health Behaviors in University and College Staff: A Systematic Review. Am J Health Promot. 2015;29(5):e169-e187.
- Wardle J, Haase AM, Steptoe A. Body image and weight control in young adults: international comparisons in university students from 22 countries. Int J Obes. 2006;30(4):644-651.
- Ferraro ZM, Patterson S, Chaput J-P. Unhealthy weight control practices: culprits and clinical recommendations. Clin Med Insights Endocrinol Diabetes. 2015;8:7-11.
- Park B, Cho H, Choi E, et al. Weight control behaviors according to body weight status and accuracy of weight perceptions among Korean women: a nationwide population-based survey. Sci Rep. 2019;9.
- Harring HA, Montgomery K, Hardin J. Perceptions of body weight, weight management strategies, and depressive symptoms among US college students. J Am Coll Health. 2010;59(1):43-50.
- Almaiman A, Al Wutayd O. Assessment of the Side Effects of Random Weight-loss Diet Programs (protein-based) on Health in a Saudi Community. Int. J. Pharm. Phytopharm. Res. 2019;9(6):39-46.
- Haynes A, Kersbergen I, Sutin A, Daly M, Robinson E. A systematic review of the relationship between weight status perceptions and weight loss attempts, strategies, behaviours and outcomes. Obes Rev. 2018;19(3):347-363.
- Utter J, Denny S, Robinson E, Ameratunga S, Crengle S. Identifying the ‘red flags’ for unhealthy weight control among adolescents: Findings from an item response theory analysis of a national survey. Int J Behav Med. 2012;9(1):99.
- Alfadda AA, Al-Dhwayan MM, Alharbi AA, et al. The Saudi clinical practice guideline for the management of overweight and obesity in adults. Saudi Med J. 2016;37(10):1151-1162.
- Saudi Arabia Ministry Of Health. Obesity Control Program teams. The Saudi Guidelines on the prevention and management of obesity. 2016.
- World Health Organization. Global strategy on diet, physical activity and health. 2004.
- Nour M, Lutze SA, Grech A, Allman-Farinelli M. The Relationship between Vegetable Intake and Weight Outcomes: A Systematic Review of Cohort Studies. Nutrients. 2018;10(11):1626.
- Higgs S, Thomas J. Social influences on eating. Curr Opin Behav Sci. 2016;9:1-6.
- Rounsefell K, Gibson S, McLean S, et al. Social media, body image and food choices in healthy young adults: A mixed methods systematic review. Nutr Diet. 2020;77(1):19-40.
- De Brún A, McCarthy M, McKenzie K, McGloin A. Weight stigma and narrative resistance evident in online discussions of obesity. Appetite. 2014;72:73-81.
- Wang ML, Pbert L, Lemon SC. Influence of family, friend and coworker social support and social undermining on weight gain prevention among adults. Obesity (Silver Spring, Md). 2014;22(9):1973-1980.
- Freeman B, Kelly B, Baur L, et al. Digital junk: food and beverage marketing on Facebook. Am J Public Health. 2014;104(12):e56-e64.
- Freeman B, Kelly B, Vandevijvere S, Baur L. Young adults: beloved by food and drink marketers and forgotten by public health? Health Promot Int. 2016;31(4):954-961.
- Gosadi IM. National screening programs in Saudi Arabia: Overview, outcomes, and effectiveness. J Infect Public Health. 2019;12(5):608-614.
- Saudi Arabia Ministry Of Health. Obesity and Overweight. 2016; https://www.moh.gov.sa/en/HealthAwareness/EducationalContent/Diseases. Accessed 10 June, 2020.
- Santos I, Sniehotta FF, Marques MM, Carraça EV, Teixeira PJ. Prevalence of personal weight control attempts in adults: a systematic review and meta-analysis. Obes Rev. 2017;18(1):32-50.
- Richardson M, Madzima T, Nepocatych S. Differences in Body Composition Affect Weight Control Practices and Body Image Satisfaction in College Students. PAAH. 2019;3(1):1-10.
- Tol J, Swinkels IC, De Bakker DH, Veenhof C, Seidell JC. Overweight and obese adults have low intentions of seeking weight-related care: a cross-sectional survey. BMC Public Health. 2014;14(1):582-582.
- Stephen EM, Rose JS, Kenney L, Rosselli-Navarra F, Weissman RS. Prevalence and correlates of unhealthy weight control behaviors: findings from the national longitudinal study of adolescent health. J Eat Disord. 2014;2(1):16.
- Mond J, Hay P, Rodgers B, Owen C, Crosby R, Mitchell J. Use of extreme weight control behaviors with and without binge eating in a community sample: Implications for the classification of bulimic‐type eating disorders. Int J Eat Disord. 2006;39(4):294-302.
- Keogh A, Chadwick B. Health food blogger: friend or foe? Br Dent J. 2019;227(12):1051-1057.
- van Baak MA, Mariman ECM. Dietary Strategies for Weight Loss Maintenance. Nutrients. 2019;11(8):1916.
- Soeliman FA, Azadbakht L. Weight loss maintenance: A review on dietary related strategies. J Res Med Sci. 2014;19(3):268-275.
- Cox CE. Role of Physical Activity for Weight Loss and Weight Maintenance. Diabetes Spectr. 2017;30(3):157-160.
- Blundell JE, Gibbons C, Caudwell P, Finlayson G, Hopkins M. Appetite control and energy balance: impact of exercise. Obes Rev. 2015;16 Suppl 1:67-76.
- Ganesan K, Habboush Y, Sultan S. Intermittent Fasting: The Choice for a Healthier Lifestyle. Cureus. 2018;10(7):e2947-e2947.
- Harris L, Hamilton S, Azevedo LB, et al. Intermittent fasting interventions for treatment of overweight and obesity in adults: a systematic review and meta-analysis. JBI Database System Rev Implement Rep. 2018;16(2):507-547.
- Horikawa C, Kodama S, Yachi Y, et al. Skipping breakfast and prevalence of overweight and obesity in Asian and Pacific regions: a meta-analysis. Prev Med. 2011;53(4-5):260-267.
- Ledoux TA, Hingle MD, Baranowski T. Relationship of fruit and vegetable intake with adiposity: a systematic review. Obes Rev. 2011;12(5):e143-e150.
- Majeed F. Association of BMI with diet and physical activity of female medical students at the University of Dammam, Kingdom of Saudi Arabia. J Taibah Univ Sci. 2015;10(2):188-196.
