
Low Back Pain, Disability and Quality of Life among Health Care Workers
Nehad Ahmed Ibrahim Zahra1,2*, Eman Ali Abd Elmoaty Sheha3, Hanan Abdelwahab Elsayed2
1Assistant prof. Assistant Medical Science Department, Community College, Tabuk University, Saudi Arabia,
2Assistant prof. Community Health Nursing, Benha University, Benha, Egypt.
3Lecturer of Community Health Nursing, Faculty of Nursing, Fayoum University, Egypt.
ABSTRACT
Health workers usually have the highest incidence of work-related back injuries which influence their work. Low back pain patients suffer not only from physical discomfort but also from functional disabilities that may cause impairment and interfere with their quality of life. This study is aimed at evaluating low back pain, disability and quality of life among health care workers. This is a descriptive study which was conducted at four primary health care centres in Tabuk. Non-probability purposive sampling method was used to select 120 health workers. For data collection, the three tools used were a pre-established questionnaire, Oswestry Low Back Pain Disability Questionnaire for evaluating pain and disability, and the 36-item Short-Form Health Survey (SF-36) for evaluating the quality of life. Disability was found in 70.8% of the studied sample. Total quality of life score was low in 77.5% of the studied sample and there was a highly significant negative correlation between total quality of life score and total back pain of the studied sample. Low back pain continues to be a common occupational disease for health workers. This health issue would also have an important impact on their job and the quality of healthcare as well. In order to decrease Low back pain, health care workers should be included in specific education program. A consistent methodological strategy for optimizing the qualiy of life problem among health care workers should be developed by health care managers.
Key words: low back pain, disability, health workers, quality of life.
INTRODUCTION
Low back pain (LBP) is one of the musculoskeletal occupational disorders for health care workers world wide. This is one of the most common musculoskeletal issues. Several studies showed a higher prevalence of LBP among medical practitioners than any other symptoms. [1]
LBP refers to the dorsal pain that is between below the costal margin and above the curve of the gluteal and can spread to legs. LBP is a major public health problem, can lead to job losses, severe financial losses and numerous physical and psychological issues because of its chronic nature. [2]
Health care workers are at the risk of having LBP due to their profession's physical and emotional factors. Health care workers often experience low back pain at a rate that exceeds that of construction, mining, and manufacturing workers. These injuries are mostly due to repeated manual patient handling, involving heavy manual lifting associated with transferring, patient repositioning and working in extremely difficult postures [3, 4].Long working hours, excessive workload, inadequate staff and equipment, inadequate breaks, standing up for long periods of time, working in a wrong position, disturbing the sleeping cycle and eating habits due to shifts are among the occupational risk factors that can lead to LBP in health care workers [5].
Quality of life is the general well-being of individuals and communities, outlining negative and positive aspects of life. It observes life satisfaction, including all aspects from physical health, family, education, employment, wealth, safety, security to freedom, religious beliefs, and the environment [6].
Quality of life (QOL) has become an important factor for health care providers and patients with acute and chronic health conditions which has many aspects including physical, financial, spiritual and psychological ones [7].
In general, it can be pointed out that back pain affects all aspects of life leading to lowers quality of life (QOL). Therefore, what is important in the treatment and care of chronic diseases such as back pain, in addition to disease control, is improving the quality of life and issues such as social restrictions, physical and health problems caused by back pain that are QOL assessment factors as well as discovering other difficulties related to QOL which is helpful in the treatment process [8]. Limited studies have examined quality of life for health care workers. They have been generally ignored when addressing low back pain; therefore, this study aimed to evaluate low back pain, disability and quality of life among health care workers.
Research questions
The main aim of the study is to address the following research questions:
Significance of the study:
Low back pain (LBP) is one of the most common occurring occupational musculoskeletal diseases among all health care workers. LBP ranks the second reason for loss of workforce and health expenses following cancer pain that leads to significant loss of function and reduces the quality of life. In addition, 50-85 per cent of the world's population is experiencing LBP at some point in their lifetime [5]. Prevalence increases and reaches the peak at the age range of 35 to 55 years old. 3.55 of nurses are estimated to leave their profession due to back pain. Low back pain is a common health problem among health care workers who work in Taif operating rooms. This is a leading cause of temporary disability [9]. In Egypt, LBP prevailed that 79.3% of the studied group of working nurse in Zagazig University Hospitals[10] and common among Egyptian Physical therapists in the teaching hospitals in Cairo[11]. The prevalence of LBP amongst Saudi is around 18.8%; while, the prevalence of LBP amongst healthcare providers in Makkah is 74.2% and in eastern region in Saudi Arabia the majority of healthcare workers experience LBP in their lifetime with highest rate in nurses [12].
SUBJECTS AND METHODS:
Research Design:
- This is a descriptive cross-sectional design.
Setting:
This study was conducted at four primary health care centers in Tabuk which were Alnahda, Alsaada, Alworood and Almoroj centers.
Sample:
Multi stage (cluster) random sampling method was used to choose 25% of primary health centers, and the health care workers were selected using non-probability purposive sampling method. Inclusion criteria were the workers who were free from psychiatric disorders, cancer, arthritis or any other inflammation diseases of the spine and spinal surgery and accepted to participate in the study. The expected number of subjects was calculated by the following formula:

Where n is the sample size, N is the population, and e is the margin error (0.05).
Tools of Data Collection:
Three tools were used in the study including a pre-established questionnaire the researchers developed it after reviewing the related literature. It was written in Arabic and composed of close-ended questions. It consisted of socio-demographic data of health care workers including age, gender, education, occupation, years of experience and history of low back pain and disability.
The second tool was Oswestry Low Back Pain Disability Questionnaire which was used to assess low back pain and disability. This questionnaire has been designed to give information as how back or leg pain affects the ability to manage in everyday life. The test is considered as the ‘gold standard’ of low back functional outcome [13].
The third tool was a 36-item Short-Form Health Survey (SF-36) which was used to assess the quality of life. This questionnaire is a reliable and valid internationally and has 36 questions in 8 dimensions as physical function, role limitations due to physical function, bodily pain, general health vitality, and mental health; and role limitations due to psychological and social functioning. Based on the available instructions, raw scores of eight areas of quality of life related to health are calculated and then turned to a standard score between zero to one hundred. The higher value means the better condition [14].
Content validity:
The methods were presented to a panel of five public health nursing experts to determine the quality of the content. Panel judgment on the meaning of the sentences and the appropriateness of the content were revised.
Pilot study:
A pilot study was carried out on about 10% of the sample, who were excluded from the study sample. The contents, clarity, accuracy and applicability of the instruments were randomly evaluated using the interview questionnaire. Modifications were therefore produced to the research instruments in order to be more relevant and the needed modifications were accomplished by correcting, omitting or adding objects until the final shape of the instruments was reached. It also helped forecast the time it took for data to be collected. After undertaking the pilot survey, it was discovered that the phrases of the instruments were clear and meaningful, but few words were altered according to the pilot study outcomes.
Fieldwork:
Data collection was from the end of September 2019 to the end of November 2019. The researcher and assistant for health workers in the selected setting carried it out. Those health care workers who fulfilled the selection criteria enrolled in the study and asked to fill out a questionnaire and marked their responses to the data sheet. Each health care worker takes approximately, 35-40 minutes to complete it. Health care workers were interviewed during study time in their departments from 9 Am to 1 Pm 3 days weekly.
Ethical considerations:
At the beginning, the purpose of the study and the tools used in it were approved by the Permanent Local Committee for Research Ethics at the University of Tabuk. All health care workers rights were secured, and informed about the nature of the expected outcomes of the study. They were assured that all data will be confidentially tested and information will be used for the research purpose only for their benefits and each study subject was allowed time enough throughout the study. They were also informed about their right of withdrawal at any time without expressing any reasons. And finally, they signed the approval form.
Statistical design:
Data entry, presentation, and statistical analysis were done using the Statistical Package for Social Science (SPSS) version 13 on IBM compatible computer. Quantitative data were expressed as means and standard deviations and analysed using paired student t-test to test the difference between two groups of the same sample of normally distributed variables. Qualitative data were expressed as numbers and percentages (No & %) and analysed using McNamara test to test the difference between two or more groups of the same sample. Significant results were considered as follows: P ≤ 0.05 Significant, р > 0.05, Not significant, and P ≤ 0.001 Highly significant.
RESULTS:
Table 1: Distribution of the Demographic Characteristics of the Studied Sample (N=120)
|
Personnel characteristics |
Frequency |
% |
|
Age In years |
||
|
25-<35 |
79 |
65.8 |
|
35-<45 |
25 |
20.8 |
|
45-55 |
16 |
13.4 |
|
Mean ±SD |
31.61±8.65 |
|
|
Gender |
|
|
|
Male |
84 |
70.0 |
|
Female |
36 |
30.0 |
|
Educational qualification |
||
|
Secondary |
61 |
50.8 |
|
University |
29 |
24.2 |
|
Postgraduate |
30 |
25.0 |
|
Nationality |
|
|
|
Saudi |
26 |
21.7 |
|
Non-Saudi (Egyptian & others) |
94 |
78.3 |
|
Job |
|
|
|
Doctor |
23 |
19.2 |
|
Nurse |
31 |
25.8 |
|
Heath worker |
66 |
55.0 |
|
Years of experience |
||
|
1-<5 years |
10 |
8.3 |
|
5-<10 |
82 |
68.3 |
|
≥10 |
28 |
23.4 |
|
Mean ±SD |
8.56±5.39 |
|
Table 1 show that the mean age of the studied sample was about 31.6±8.65. 70% of them were male, educational qualification of about slightly more than half of them was secondary education, the majority of the studied sample (78.3%) were Egyptian health care workers & other nationalities (non-Saudi). The mean years of experiences of them were 8.56±5.39.
Table 2: Distribution of Intensity of Low Back Pain among the Studied Sample (N=120)
|
Dimension |
Minimum |
Maximum |
Mean ±SD |
% of mean score |
|
Pain intensity |
1.00 |
4.00 |
2.74 ±.90 |
54.8 |
|
Personal care (washing, dressing, etc.) |
1.00 |
4.00 |
2.92 ±.80 |
58.5 |
|
Lifting |
2.00 |
4.00 |
2.90 ±.73 |
58.0 |
|
Walking |
2.00 |
4.00 |
2.80 ±.736 |
56.1 |
|
Sitting |
1.00 |
4.00 |
3.07 ±.76 |
61.5 |
|
Standing |
1.00 |
4.00 |
2.90 ±.86 |
58.1 |
|
Sleeping |
1.00 |
4.00 |
2.70 ±.80 |
54 |
|
Sex life (if applicable) |
2.00 |
4.00 |
2.46 ±.64 |
49.3 |
|
Social life |
1.00 |
4.00 |
2.60 ±.79 |
52.0 |
|
Travelling |
1.00 |
4.00 |
2.69 ±.77 |
53.8 |
Table 2 show that the distribution of the mean score of low back pain intensity among the studied sample was 61.5% in sitting, 58.5% in personal care such as washing, dressing, etc., and 58.1% and 58% in standing and lifting, respectively.
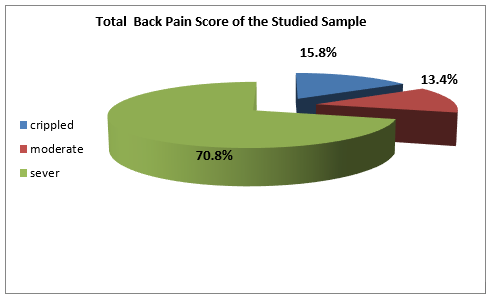
Figure 1: Distribution of Total Back Pain Score of the Studied Sample
Figure 1 show that the total back pain score of the studied sample was sever back pain in 70.8% of the studied sample, and was crippled in 15.8% of them, and 13.4% of them reported that the score was moderate back pain.
Table 3: The Relationship Between Intensity Total Low Back Pain Score and Demographic Characteristics of the Studied Sample (N=120)
|
Demographic Characteristics |
Total back pain score |
||
|
Frequency |
F/independent t test |
P value |
|
|
Age In years |
|
74.50 |
<0.001** |
|
25-<35 |
26.21±2.47 |
|
|
|
35-<45 |
30.08 ±.40 |
|
|
|
45-55 |
32.18 ±1.10 |
|
|
|
Gender |
|
12.43 |
<0.001** |
|
Male |
26.80 ±2.64 |
|
|
|
Female |
31.46 ±1.30 |
|
|
|
Educational qualification |
|
129.76 |
<0.001** |
|
Secondary |
25.39 ±2.22 |
|
|
|
University |
29.34 ±.48 |
|
|
|
Postgraduate |
31.26 ±1.31 |
|
|
|
Nationality |
|
13.45(t) |
<0.001** |
|
Saudi |
26.34 ±2.51 |
|
|
|
Non-Saudi (Egyptian & others) |
31.00 ±1.27 |
|
|
|
Job |
|
219.58 |
<0.001** |
|
Doctor |
23.13 ±1.86 |
|
|
|
Nurse |
26.48 ±.769 |
|
|
|
Heath worker |
30.07 ±1.49 |
|
|
|
Years of experience |
|
115.53 |
<0.001** |
|
1-<5 years |
21.60 ±1.83 |
|
|
|
5-<10 |
27.36 ±1.94 |
|
|
|
≥10 |
31.35 ±1.31 |
|
|
Table 3 shows that there were highly significant relationship between intensity of total low back pain score and all aspects of demographic characteristics (age, sex, educational qualification, nationality, job and years of experience).
Table 4: Distribution of the Quality of Life of the Studied Sample (N=120)
|
Dimension |
Minimum |
Maximum |
Mean ±SD |
% of mean score |
|
physical functioning |
.00 |
1000.00 |
365.83±335.37 |
36.58 |
|
role limitation physical |
.00 |
400.00 |
208.33 ±121.32 |
52.08 |
|
Role limitation emotional |
.00 |
300.00 |
185.00 ±99.28 |
61.66 |
|
Energy fatigue |
.00 |
320.00 |
207.16 ±82.88 |
51.79 |
|
Emotional well being |
.00 |
400.00 |
253.50 ±158.10 |
50.7 |
|
Social function |
100.00 |
200.00 |
147.50 ±30.98 |
73.75 |
|
Pain |
.00 |
110.00 |
56.20 ±32.17 |
28.104 |
|
General health |
.00 |
300.00 |
116.25 ±85.35 |
23.25 |
|
Total quality score |
900.00 |
2810.00 |
1539.79 ±400.88 |
48.11 |
Table 4 shows that the distribution of the mean score of total quality of life among the studied sample was 73.75% in social function, 61.66% in role limitation emotional, 52.08% in role limitation physical, and 51.7% in energy fatigue.
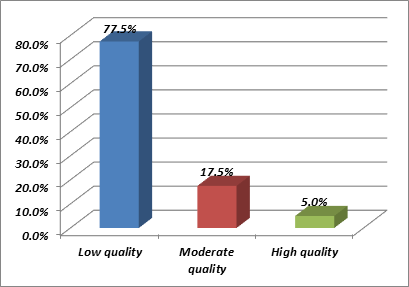
Figure 2: The Distribution of the Total Quality of Life Score of the Studied Sample
Figure 2 shows that the total quality of life score was low in 77.5% of the studied sample, moderate in 17.5% and high in only 5.0%.
Table 5: The Relationship between Total Quality of Life Score and Demographic Characteristics of the Studied Sample (N=120)
|
Demographic Characteristics |
Total quality of life score |
||
|
Frequency |
F/independent t test |
P value |
|
|
Age In years |
|
61.19 |
<0.001** |
|
25-<35 |
1738.41 ±341.83 |
|
|
|
35-<45 |
1258.20 ±91.58 |
|
|
|
45-55 |
999.06 ±45.90 |
|
|
|
Gender |
|
14.91 |
<0.001** |
|
Male |
348.77 ±35.97 |
|
|
|
Female |
98.92 ±19.40 |
|
|
|
Educational qualification |
|
118.07 |
<0.001** |
|
Secondary |
1094.66 ±124.40 |
|
|
|
University |
1351.03 ±28.70 |
|
|
|
Postgraduate |
1848.44 ±312.63 |
|
|
|
Nationality |
|
13.07(t) |
<0.001** |
|
Saudi an |
1724.20 ±343.37 |
|
|
|
Non-Saudi an |
1141.84 ±144.03 |
|
|
|
Job |
|
258.19 |
<0.001** |
|
Doctor |
2173.47 ±230.29 |
|
|
|
Nurse |
1691.93 ±130.60 |
|
|
|
Heath worker |
1247.50 ±168.89 |
|
|
|
Years of experience |
|
126.2 |
<0.001** |
|
1-<5 years |
2369.50 ±213.72 |
|
|
|
5-<10 |
1595.73 ±255.56 |
|
|
|
≥10 |
1079.64 ±114.51 |
|
|
Table 5 shows that there was a highly significant relationship between total quality of life score and all aspects of demographic characteristics (age, sex, educational qualification, nationality, job and years of experience).
Table 6: Correlation of Total Quality of Life Score level and Total Back Pain of the Studied Sample (N=120)
|
Variables |
Low Back Pain |
|
|
Quality of life |
r |
P value |
|
|
-.652** |
<0.001** |
Table 6 shows that there was a highly significant negative correlation between total quality of life score and total back pain of the studied sample.
DISCUSSION:
Low back pain (LBP) is a highly prevalent health problem that is responsible for extreme discomfort and impairment relative to any other worldwide health condition. Healthcare workers are at risk of having LBP because of the physical and emotional aspects of their occupation. The aim of this study was to evaluate low back pain, disability and quality of life among health care workers.
According to demographic characteristics of the participants, the study indicated that the mean age of studied sample was 31.6±8.65. The majority of them were male, we included both male and female in the study at the request of the management of the selected health centres due to the importance and spread of the problem among health care workers of both sexes. The educational qualification of the studied sample was secondary in about slightly more than half of them. The majority of the studied sample was non-Saudi as Egyptian and other nationalities. Saudi Arabia vision 2030 aims to increase the Saudi in health care sector by equipping them with essential knowledge and skills needed. The mean years of experiences of them was 8.56±5.39, this suggests that longer working hours may be associated with higher LBP prevalence.
Concerning to the distribution of the mean score of low back pain intensity among the studied sample, the most of the studied sample aggravated low back pain with sitting position, personal care such as washing, dressing, etc., standing position and lifting objects. This is in accordance with the study that was conducted in Bangladesh among adult LBP patients [15]. The study revealed that (16.1%) of cases’ long standing and weight lifting aggravated back pain.
It was reported that there is a significant relationship between physical factors and musculoskeletal problems. Repetitive movements, improper posture and excessive use of force are the three main factors which lead to musculoskeletal problems. Such factors lead to overuse of tendons, ligaments and muscles, repetitive muscle loading and fatigue, thus increasing the likelihood of low back trauma. Carrying out duties without assistive medical equipment can also lead to LBP [16].
According to health workers, specific job tasks such as supporting the daily lives of patients, putting them on the beds, holding and moving them or transporting medical devices of different weights and sizes often increase the risk of low back injuries. American Nurses Association (ANA) stated that the duties of nurses that require carrying patients are related with LBP[17, 18].this was supported by the finding of study that conducted on surgical nurses [19] who found that carrying a patient to another bed / stretcher is the factor that most often causes LBP. The literature indicates that nursing practices are risk factors in LBP development.
It had been suggested that getting support/help during nursing care practices is correlated with LBP. Also, this point of view was in agreement with the findings of the study conducted by Ovayolu et al. 2014 [20] who found that conducting certain nursing practices without help/getting support from an equipment increases the frequency and intensity of LBP. It reflects the urgent need for self-back care intervention educational program.
The results of the current study reveal that sever disability was found in the majority of the studied sample, while, the minority of them reported that crippled and moderate disabilities. Our results are in accordance with the result of another study [15] which found that nearly two-third of low back pain patients had severe pain on the back; moreover, one-third of the patients felt moderate pain and few of them felt mild pain on the back. However, these previous findings were in contrast to the finding of another study conducted by Nujhat [21] who found dissimilar results that among participants, the severity of VAS-scale pain was 29.6% having no pain, 58.3% medium pain, and 12.20% severe pain. Also, Among LBP respondents in the study which was reported in Southwestern Nigeria, 68% described their pain as mild, 20% as moderate, and 12% as severe [22].
In a cross-sectional survey of LBP, among 1,600 health care workers in 6 Turkish hospitals in 4 cities including nurses, doctors, physical therapists, technicians, secretaries and hospital assistants, 63% of the respondents described their pain as moderate, 23.1% as severe, and 11.1% as mild. [23] 42.8% of the respondents indicated that LBP disrupted their sleep in the study conducted by Johnson and Edward [24]. Multiple studies have recorded high prevalence of sleep disturbance among LBP patients, and sleep disruption was found to be dependent on pain intensity [25, 26]. Pain is a subjective feeling, because different people react in different ways to the pain.
The present study shows that there were a highly significant relationship between total score level of low back pain and all aspects of demographic characteristics. Our results are in consistence with the finding of Kehinde et al. [27], who concluded that the various factors (individual, occupational and psychosocial) have been shown to be correlated with LBP. Older age has been shown to be associated with increased incidence of low back pain. Individuals aged between 20 and 29 years had a prevalence of low back pain of 31% which was found to increase to 73.5% for those aged between 50 and 59 years. This finding are in consistence with Multivariate analysis stressed that older age as an independent risk factor for LBP in the study carried out by Cunningham et al.[28] Johnson and Edward [24] also noted a higher prevalence of LBP among respondents over 35 years of age, compared with a lower prevalence in those under 35 years of age.They also established that longer working hours was associated with higher LBP prevalence. This result was also corroborated by the research carried out by Hinmikaiye and Bamishaiye [19] they found that the respondents who worked for over 8 years had a higher prevalence of LBP; while, those who worked for under 2 years had a lower prevalence of LBP. Similarly, Gebrehiwot et al. [29] reported that health care workers who served for more than 12 years had a higher prevalence of LBP than those who worked for less than 12 years.
The results of the current study reveal that low total quality of life score level in the majority of the studied sample, while, moderate in 17.5% of them and high in only 5.0% of the studied sample. Higher total mean score level of quality of life of the studied sample according to dimensions in social function, role limitation emotional, role limitation physical, and energy fatigue. LBP can affect patients ' quality of life, as pain alone can reduce their work output and affect their social life.
Tthis point of view was in agreement with the findings of a quasi-experimental study among adult LBP patients, a self-care intervention was applied to compare QOL of patients with low back pain before and after the intervention using SF-20 scale. It was found that regarding the level of quality of life of low back pain (LBP) patients, after the intervention (7.1%) had good QOL and good quality of life was absent before the intervention. In addition, the mean QOL before the intervention was (44.6%). It also found that (55.4%) of them low back pain patients had poor quality of life. The mean score of physical function among low back pain patients was 33.02 ±18.32before the self-back care intervention [19].
In the same line, our results agreed with the findings of another a cross-sectional study of health-related quality of life (HRQOL) in patients with low back pain in ambulatory clinics found that HRQOL and pain severity mean was 64.0 (15.9) and 52.6 (21.8), respectively [30]. Body pain subscale SF-36 was found to be the most responsible factor to changes in LBP patients in other previous studies [31].
The results of the present study showed that there was a highly significant relationship between total quality of life score and all aspects of demographic characteristics. This explained that the education is a main factor to help people to live better; it was not surprising for us to find that health workers with a higher education might experience a higher HRQOL score. Meanwhile, there were many studies reporting that patients with a higher education experienced less severity of LBP and disability [30] and our study corroborates the above phenomenon. Also in another study which investigated that the effects of socio-demographic factors on quality of life in women living in Lublin Province in Poland, it was indicated that the socio-demographic data of women is correlated with their quality of life score [32].
Also, This may be due to the experience years gives the health care workers more skills and competence, and it may help them improve their health and increase their quality of life. People with higher education and with more working experience are more aware of preventive measures for chronic conditions and they may have a positive attitude towards lifestyle changes.
This results conveying and confirming that there was a highly significant negative correlation between total score level of life quality and total back pain score level of the studied sample. This point of view was in agreement with the findings of numerous studies having reported a significant decline in the quality of life among nurses with work-related LBP among nurses. This consequence would also have an important impact on the work of the nurses and the quality of healthcare [33].
Similary, another study was carried out by 122 nurses at the Clinical Practice and Research Hospital to study the effects of low back pain on quality of life and functional impairment in low back pain nurses [34].The nurses who had more pain intensity had significantly worse scores of functional disability general health, physical function, role physical, social function and bodily pain domains of SF-36 compared to nurses who had less pain intensity.
Importantly, both physical and mental health is linked with chronic back pain. The back pain is associated with reduced quality of life; and a significant relationship with chronic back pain was found among all measures of physical and mental health [35].Such findings also agree with the results of the 2001 National Survey in Spain using the Health Assessment Questionnaire (HAQ) and SF-12 instruments, according to which lower back pain significantly deteriorates the quality of life and work [36]. In fact, chronic back pain shows similar impairment in mental health and greater physical disability when compared with bipolar disorder [37].
CONCLUSION
Based on the results of this study, LBP remains a serious occupational illness for health care workers. This health problem would also have a significant effect on their job and a great impact on the quality of life of the health care workers. These findings can be used as an important guide for health care managers to include specific education programs designed to reduce LBP among health workers. It may also be used to formulate a simple methodological approach to optimize the QOL problem among health care workers.
Recommendation:
Based on the results of the present study, the following recommendations are suggested:
ACKNOWLEDGEMENTS
REFERENCES

