Leaves of Capparis cartilaginea Exhibit a Promising Antidiabetic Activity in Alloxan-Induced Diabetic Rats
Bushra Abdulkarim Moharram1*, Hassan M. AL-Mahbashi2, Tareq Al-Maqtari1, 3, Riyadh Saif-Ali4, Ibrahim Ali Al-Hakami1, Wahibah Taher Alhaj1
1Department of Pharmacognosy, Faculty of Pharmacy, Sana’a University, Sana’a, Yemen.
2Department of Forensic Medicine and Clinical Toxicology, Faculty of Medicine, Sana’a University, Sana’a, Yemen.
3Department of Pharmaceutical Sciences, College of Pharmacy and Allied Health Professions, South Dakota State University, Brookings, SD, USA.
4Department of Biochemistry and Molecular Biology, Faculty of Medicine, Sana’a University, Sana’a, Yemen.
*Email: [email protected]
ABSTRACT
Diabetes Mellitus (DM) is among the most common metabolic disorders worldwide. Leaves of Capparis cartilaginea are used in folk medicine to treat diabetes in parts of Yemen. The current study aimed to investigate the antioxidant and antidiabetic effects of C. cartilaginea leaf extract. The antioxidant activity of the extract was determined using a 2.2 – diphenyl -1- picrylhydrazyl (DPPH) free radical scavenging assay. Experimental diabetes was induced in rats by alloxan (200 mg/kg), and animals with fasting blood glucose levels>200 mg/dL were considered diabetic. On day 14 post-treatment with the plant extract, body weight, fasting blood glucose, high-density lipoprotein (HDL), low-density lipoprotein (LDL), total cholesterol, and triglyceride (TG) levels were determined for serum samples. The in vitro α-amylase inhibition assay was performed using an α-amylase-based kit. The leaf extract exhibited a pronounced antioxidant effect as evidenced by an IC50 value of 187.36 µg/ml. The C. cartilaginea-treated animal groups showed a significant reduction in blood glucose levels compared to day one of treatment (P < 0.05). The extract at a dose of 200 mg/kg caused a significant decrease in the levels of LDL, cholesterol, and TG, and induced an increase in HDL (P < 0.05-0.01). The plant extract exhibited modest α-amylase inhibition with an IC 50 value of 861.3 μg/mL. The results provide evidence that C. cartilaginea may be a promising adjunct therapeutic tool for the management of diabetes and its associated hyperlipidemic complications.
Key words: C. cartilaginea leaves, Fasting blood sugar, Lipid profile, Alloxan-induced diabetes, α-amylase
INTRODUCTION
Diabetes mellitus results in a hyperglycemic state driven by insulin being deficient or largely unable to function. Its symptoms also include hyperlipidemia and alterations in protein metabolism [1]. Untreated cases may result in macro-vascular and micro-vascular manifestations which can cause multiple organ failures, particularly in the kidneys, retina, and nervous system [2]. Diabetes treatment relies mainly on stimulating insulin secretion from beta cells in the pancreas, sensitizing target tissues to insulin, or inhibiting the absorption of oligo-saccharides [3, 4].
Plants have been and are still important sources of therapeutic agents that could be utilized in the treatment of various illnesses, among which is diabetes [5, 6]. It is estimated that the majority of people living in the non-developed world use plant-based preparations in their traditional healthcare systems to treat various diseases [7]. Part of the global interest in the utilization of natural medicinal plants is fueled by the complexity, adverse effects (e.g. lactic acidosis, severe hypoglycemia, and gastrointestinal distress…..etc), and high cost associated with available conventional medications [5, 8].
C. cartilaginea Decne, (family Capparidaceae) is used in some countries for diabetes, rheumatic fever, worms [9], bruises, earache, headache, snakebites, swelling, and to ease maternal labor [10]. Phytochemical analyses of the plant have led to the isolation of flavonoids [11, 12], isothiocyanates [10, 13], Kaempferol, Dihydroxy-lup-20(29)-en-28-oic acid, and β-sitosterol [14]. Other phytochemical constituents have also been identified such as alkaloids, carbohydrates, saponins, polyphenols, tannins, coumarins, phytosterols, bitter principles, triterpenes, amino acids, and proteins [13, 15]. Therapeutically, multiple pharmacological properties have been reported for C. cartilaginea such as antibacterial, anti-ulceration, antioxidant, cytotoxic, larvicidal, antimicrobial, anti-inflammatory, hypotensive, and bradycardiac effects [13, 15-17].
Based on the ethnobotanical use of C. cartilaginea leaves, we sought in this work to assess the in vitro as well as the in vivo hypoglycemic potential of C. cartilaginea extract on diabetic rats. Based on available literature, no studies have investigated the anti-diabetic potential of C. cartilaginea.
MATERIALS AND METHODS
Equipment
Buchirotavapour R-215 (Switzerland), equipped with Buchi water bath B-491 and a Buchi v-700 vacuum system, was used to dry C. cartilaginea leaves ethanolic extract. Microtiter readers (Linear GEA, Spain) were used for the antioxidant activity assay. For the antidiabetic activity determination, the following equipment was used: a centrifuge (Hermle Z400, Germany), a chemistry analyzer model BS-240 (Mindray, China) for the α-amylase inhibitory assay, and a spectrophotometer (Shimadzu UV-1650 PC) to measure total phenolic content.
Chemicals and reagents
Methanol (Umco, Egypt), 96% ethanol (Umco, Eygept), and 2,2-diphenyl-1-picrylhydrazyl (DPPH; Sigma, Germany) were utilized to assess the antioxidant activity. Folin-Ciocalteu reagent (Labo Chemie, India), Galic acid (GA) (Labo Chemie, India), and sodium carbonate (NaCO3) (BDH, England) were used to determine the phenolic content. Daonil® containing glibenclamide as the active ingredient (Sanofi, Egypt), Garbose containing 100 mg acarbose (YSP, Malaysia), alloxan 98% (Oxford laboratory, India), bacterial α-amylase (BDH, UK) were used for antidiabetic analyses. The α-amylase-EPS (BioSystems S.A., Spain) acting as a substrate contained reagent A and regent B (Reagent A: 2 x 60 mL. HEPES 50 mmol/L, calcium chloride 0.075 mmol/L, sodium chloride 90 mmol/L, magnesium chloride 13 mmol/L, α-glucosidase > 4 U/mL, pH 7.1. Reagent B: 2 x 15 mL. HEPES 50 mmol/L, 4-Nitrophenyl-maltoheptaoside-ethylidene 18 mmol/L, pH 7.1).
Animals
Twenty-five rats (weight: 200-250 g) were kept in steel cages under a regulated 12-hour day/night cycle with controlled ventilation, humidity, and temperature (24 ± 3 °C). The rats were provided with standard pelleted feed and water ad libitum. The rats were acclimatized to the laboratory environment for a week before experimentation. The experiments on rats were carried out in accordance with the guidelines for the care and use of laboratory animals set by the National Research Council of Yemen. Approval from the ethical committee of the College of Medicine, Sana’a University was obtained (No. 15-2/8/2021).
Plant material
The leaves of C. cartilaginea (voucher specimen CC21) were harvested during the flowering season from District Kohlan Al Sharaf (Hajah governorate, Yemen) in August 2021 and were identified with the aid of Dr. Abdul Wali Al Khulaidi (Representing the public authority for research and agricultural extension, Dhamar town, Yemen).
Preparation of ethanol extract
The leaves were dried in the shade for one week, before grounding into fine powder via a blender. The dried powder (1930 g) was extracted with 96% ethanol for three days. The ethanolic extract was subject to passing through filters before the drying process started via a rotary evaporator. The percentage yield of ethanol extract was recorded based on the original dry weight (2.2%).
Preliminary phytochemical screening
Alkaloids, glycosides, carbohydrates, anthraquinones, fixed oils/fats, diterpenes, carotenoids, phenols and tannins, flavonoids, proteins, saponins, phytosterols, and coumarins were screened according to phytochemical tests described previously [18, 19].
Total phenolic content (TPC)
TPC for C. cartilaginea leaf extract was measured using the Foline Ciocalteu reagent-based assay with some modifications [20]. Briefly, 1 mg/ml of both the extract and gallic acid (GA) samples were prepared in methanol before dilution to a concentration of 50 µg/ml with distilled water. Serial dilutions of GA were then prepared (10-50 µg/ml). One milliliter of the extract or the GA solutions was added to 0.5 ml of the Folin Ciocalteu reagent followed by incubation for 5 minutes. Subsequently, 5% NaCO3 solution (2.50 ml) was added, and mixed thoroughly before incubation for 40 minutes. Absorbance at 725 nm wavelength was recorded via a spectrophotometer. All tests were done in triplicates. The TPC of the extract was expressed as mg of gallic acid equivalents (GAEs) per one gram of dry extract.
Assessing the antioxidant activity
The antioxidant potential for the C. cartilaginea methanolic extract was performed according to a previous study [13] using the DPPH radical scavenging assay. Briefly, serial dilutions of methanolic C. cartilaginea extract were prepared (62.5, 125, 250, 500, 1000, and 2000 μg/ml). From each solution, 100 μl were mixed with an identical volume of a 0.1 mmol DPPH-prepared solution in a well of a microtiter plate. This resulted in obtaining final serial concentrations of 31.25, 62.5, 125, 250, 500, and 1000 μg/ml. The plates were let to shake well for 1 minute and then left aside for 30 minutes. After that, a spectrophotometer was used to measure the absorbance at a wavelength of 492 nm. The absorbance correlates with the amount of DPPH reduced by the extract. A vitamin C solution (50-1.7 μg/ml) served as a control solution. The formula below was used to calculate inhibition:
|
% inhibition=Abc-Ab1-Ab0/Abc × 100 |
(1) |
Abc = absorbance of the control, Ab1 = absorbance of the extract with DPPH, Ab0 = absorbance of the blank (sample blank).
Antidiabetic assay (in vivo)
The antidiabetic assay was performed according to Abiola et al. [21] and Al-Baoqai et al. [22]. Albino Rats (males) were subjected to an 18-hour fasting period, before determining their fasting blood sugar (FBS) values in blood samples from the tail vein via an auto-analyzer (Accu Check Performa Advantage II, Roche). Rats were divided into five groups of five animals each. Diabetes induction in rats was performed via a single intraperitoneal injection of alloxan monohydrate (200 mg/kg). To lower the chances of severe hypoglycemia resulting from excessive insulin secretion, rats were provided for the following 24 hours with 5% glucose. A state of hyper-glycemia was seen after 3 days, confirmed by monitoring the elevation of serum glucose levels. After these 3 days, animals with serum glucose levels above 200 mg/dl were included in the study as diabetic rats. The animals were grouped into 5 groups. Group 1 were normoglycemic healthy rats (healthy control), Group 2 were diabetic but untreated rats (diabetic control), Groups 3 and 4 were diabetic rats treated with 200 and 400 mg/kg/day PO, of plant extract, respectively, Group 5 were diabetic rats treated with glibenclamide (5 mg/kg/day PO).
Treatment started three days following diabetes induction and that treatment day was considered treatment day 1. On treatment day 14, blood samples were obtained from the retro-orbital plexus with light ether-assisted anesthesia before sacrificing rats via cervical dislocation. The blood samples collected were given time to clot and then centrifuged at a speed of 3000 g for 15 min to obtain the serum. The collected serums were subject to subsequent biochemical analyses.
Determination of body weight and fasting glucose levels
Body weights and fasting serum sugar concentrations for the rats were measured before treatment and on days 7 and 14 of treatment.
Lipid profiling
Lipid parameters from animal serum samples of the experimental animals including triglycerides (TG), total cholesterol (TC), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) were measured colorimetrically using an assay kit (Mindray, China diagnostics) as per manufacturer’s instructions.
α-Amylase inhibition (in vitro study)
α-Amylase inhibition exerted by the plant extract was performed as described previously [23] with some modifications. Out of the stock methanolic solution of C. cartilaginea (100 mg/ml), 4 serial dilutions were obtained (100, 50, 25, and 12.5 mg/ml). The assay mixture contained 40 µl of plant extract from each dilution and 560 µl of methanol inside an Eppendorf tube. Blank control for each dilution of the C. cartilaginea extract was prepared by adding 40 µl of plant extract from each dilution to 760 µl of methanol. Serial dilutions of acarbose (5mg/ml), a positive control, were prepared in distilled water (D.W) to make concentrations that range between 200 and 1600 µg/ml. The assay mixture of acarbose contained 40 µl of each dilution (1600-200 µg/ml) and was mixed in 560 µl of D.W in Eppendorf tubes. The negative extract control contained methanol (40 µl) while for the negative acarbose control, 40 µl of D.W. was used.
Subsequently, a volume of 200 µl of the 2 mg/ml α-amylase solution was added to the assay mixture mentioned above (extract, acarbose, and negative control). The final volume of the assay mixture was 800 µl. The tubes underwent centrifugation for 3 minutes and then were incubated at room temperature for a total of 10 min. After that, α-amylase-ESP was added into each tube as a substrate. To determine the α-amylase inhibition for each dilution, the absorbance of liberated 4-nitrophenol at 405 nm was measured using a chemistry analyzer. The incubation mixtures had the following final concentrations: 0.625 - 5 mg/ml for the plant extract dilutions, 10 - 80 µg/ml for acarbose solutions, and 0.5 mg/ml for the 20 unit/ml enzyme.
Inhibition of α-amylase was calculated as a percentage of inhibition using the below equation:
|
Inhibition (%) = abs. of control-[abs. S-abs. B]/abs. of control ×100 |
(2) |
Where, Abs. = absorbance, abs. S = absorbance of sample, abs. B = absorbance of blank
The percentages in enzyme inhibition were plotted against the sample concentrations to establish a logarithmic regression curve, thus allowing the calculation of IC50 values. IC50 is the sample concentration (μg/ml) that would decrease α-amylase absorption by 50%.
Statistical analysis
Statistical analyses were carried out via one-way analysis of variance (ANOVA). The values were represented as mean ± standard error of the mean (mean ± SEM). Comparisons of mean values for different groups were estimated by Tukey’s multiple comparison test. A P value of < 0.05 was considered significant.
RESULTS AND DISCUSSION
Phytochemical screening
Upon phytochemical screening for C. cartilaginea leaf extract, the following chemical constituents were identified: alkaloids, carbohydrates, glycosides, saponins, diterpenes, flavonoids, anthraquinone glycosides, phenols, and tannins.
Total phenolic content and antioxidant analysis
As shown in Table 1, TPC for C. cartilaginea extract was 25.3 mg GAE/g dried extract. Also, the extract exhibited significant antioxidant potential with an IC50 value of 187.36 µg/ml (Table 1).
Table 1. Total phenolic content and antioxidant effect of C. cartilaginea leaf extract.
|
|
Total phenolic content (mg GAE/g) |
IC50 Antioxidant activity (μg/ml) |
|
leaves extract |
25.3 |
187.36 |
|
Ascorbic acid |
- |
4.36 |
GAEs = gallic acid equivalents, - = Not determined
Antidiabetic activity
Effect of C. cartilaginea leaf extract on body weight of diabetic animals
The data collected showed that the body weight of the normal non-diabetic rat group increased significantly (P < 0.05) on day 14 compared to the weight on day 1 of treatment. However, alloxan administration significantly reduced body weight (P < 0.05) of rats on day 7 and day 14 (Table 2), likely as a result of diabetes induction. Diabetic rats that were administered the C. cartilaginea extract at a 200 mg/kg dose or with glibenclamide for 14 consecutive days did not exhibit a weight reduction (P > 0.05). Interestingly, the weight of animals administered with C. cartilaginea extract at the higher dose (400 mg/kg) significantly dropped (Table 2).
Table 2. Changes in the mean body weight of alloxan-induced diabetic rats after 14 days of treatment with C. cartilaginea leaf extract
|
|
Body weight (g) |
||
|
Groups |
day 1 |
day 7 |
day 14 |
|
Normal |
203.0 ± 31.7 |
203.5 ± 28.0 |
217.8 ± 29.0* |
|
Diabetic control |
190.8 ± 21 |
170.8 ± 16.0 * |
156.3 ± 10.1* |
|
Extract-treated (200 mg/kg) |
153.8 ± 10.4 |
136.8 ± 2.7 |
163.0 ± 5.3 |
|
Extract-treated (400 mg/kg) |
245.0 ± 17.0 |
220.3 ± 19.0 * |
187.8 ± 24.2* |
|
Glibenclamide-treated |
183.0 ± 20.1 |
176.5 ± 4.8 |
168.3 ± 14.5 |
Data expressed as means ± SEMs (n = 5). *P < 0.05, **P < 0.01.
Effect of C. cartilaginea leaf extract on blood glucose levels of diabetic rats
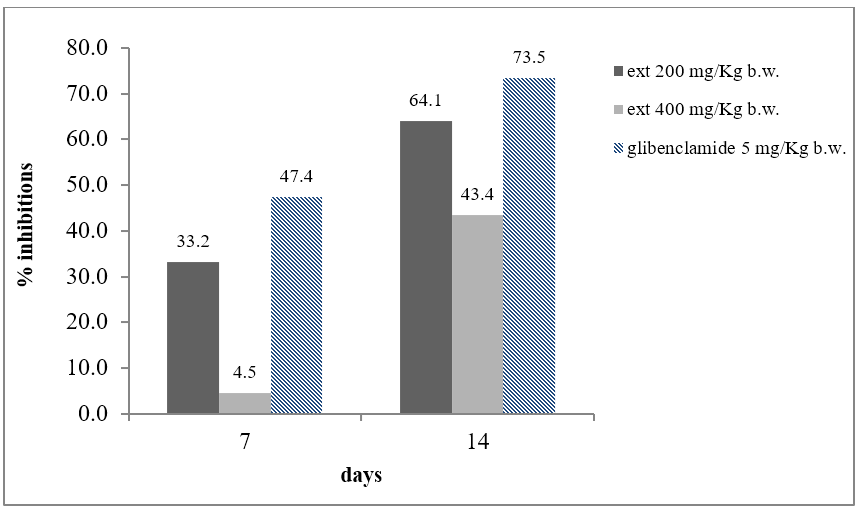
A summary of the effects of C. cartilaginea leaves on serum glucose levels in diabetic animals is shown in Table 3. As expected, on days 1, 7, and 14 of treatment, blood glucose in the diabetic control rat group (group 2) significantly increased, compared with the healthy control group 1 (P < 0.01-0.001). However, diabetic rats given C. cartilaginea extract or glibenclamide (groups 3, 4, and 5) exhibited a significant drop in blood glucose level in comparison with day one of treatment (P < 0.05-0.001). Interestingly, on day 7 post-treatment, only the animals treated with the lower dose (200 mg/kg) of the C. cartilaginea extract (group 3) showed a significant decrease in blood sugar levels (P < 0.001), while group 4 who were administered a higher dose (400 mg/kg) did not show a significant decrease in blood glucose (P > 0.05). In addition, C. cartilaginea extract at the lower dose (200 mg/kg) led to a more pronounced reduction in circulating blood glucose compared with the 400 mg/kg dose both on day 7 (33.2% vs 4.5%, respectively) and on day 14 of treatment (64.1% vs 43.4 %, respectively) (Figure 1). Interestingly, the drop in serum glucose levels induced by the 200 mg/kg extract on days 7 and 14 of treatment was similar to the drop induced by glibenclamide, a standard reference antidiabetic medication (P > 0.05).
Table 3. Effect of C. cartilaginea leaf extract on blood glucose levels in alloxan-induced diabetic rats after 14 days of oral administration.
|
|
Blood Glucose Levels (mg/dL) |
||
|
Groups |
day 1 |
day 7 |
day 14 |
|
Normal |
143.0 ± 26.0 |
103.3 ± 9.0 |
108.5 ± 4.0 |
|
Diabetic control |
579.3 ± 21.0 a*** |
480.0 ± 34.0 a** |
377.0 ± 19.0 a** |
|
Extract-treated (200 mg/kg) |
552.0 ± 28.0 a*** |
368.5 ± 21.0 b*** |
198.3 ± 0.6 b*** |
|
Extract-treated (400 mg/kg) |
409.0 ± 35.0 a*** |
390.1 ± 46.0 |
231.3 ± 27.0 b* |
|
Glibenclamide-treated |
579.0 ± 23.0 a*** |
304.8 ± 32.0 b*** |
153.8 ± 23.0 b*** |
Data expressed as means ± SEMs (n = 5). a significant compared to the respective normal group, b significant compared to respective day 1. *P < 0.05, **P < 0.01, ***P < 0.001were considered significant.
|
|
|
Figure 1. Blood glucose reduction (in percentage) induced by C. cartilaginea leaf extract and glibenclamide in alloxan-induced diabetic rats. |
Effect of C. cartilaginea leaf extract on serum lipid levels of diabetic rats
The antidiabetic effect of C. cartilaginea leaves was also observed through monitoring lipid profile changes in animal serum samples (Table 4). Upon diabetes induction, there was, as expected, a significant elevation in blood TC (P< 0.01), TG (P< 0.05), and LDL (P< 0.01) as well as a significant reduction in HDL (P< 0.05) in all diabetic groups. Interestingly, oral administration of C. cartilaginea extract (200 mg/kg) or glibenclamide was able to cause a significant decrease in total cholesterol, triglycerides, and LDL, and also induced a significant elevation in HDL levels (P< 0.05-0.01). However, rats given a higher dose of C. cartilaginea extract (400 mg/kg) did not significantly improve lipid parameters except for reducing TC in blood compared to untreated diabetic rats.
Table 4. Effect of C. cartilaginea extract on serum lipid profile parameters in alloxan-induced diabetic rats after 14 days of treatment.
|
|
lipid profile (mg/dl) |
|||
|
Groups |
Cholesterol |
TG |
LDL |
HDL |
|
Normal |
62.3 ± 3.0 |
41.5 ± 4.0 |
18.5 ± 1.6 |
51.5 ± 2.8 |
|
Diabetic control |
87.3 ± 4.0 a** |
64.3 ± 4.3 a* |
32.8 ± 1.0 a** |
42.0 ± 2.6 a* |
|
Extract (200 mg/kg) |
71.0 ± 1.0 b* |
49.5 ± 0.6 b** |
24.3 ± 0.6 b** |
56.0 ± 2.0 b* |
|
Extract (400 mg/kg) |
68.0 ± 2.5 b* |
50.8 ± 6.2 |
32.0 ± 1.6 |
41.45 ± 2.9 |
|
Glibenclamide |
55.3 ± 6.8 b** |
13.8 ± 2.0 b** |
27.0 ± 1.7 b* |
50.8 ± 3.4 b* |
Data expressed as means ± SEMs (n = 5). a significant compared to the respective normal group, b significant compared to the respective diabetic control group. *P < 0.05 and **P < 0.01 were considered significant. TG: triglycerides; TC: Total cholesterol; LDL: Low-density lipoprotein; HDL: High-density lipoprotein.
α-Amylase inhibition
The results showing α-amylase inhibition for C. cartilaginea leaf extract and acarbose (reference drug) at serial concentrations are displayed in Table 5. Both the extract and acarbose dose-dependently inhibited α-amylase. The IC50 value calculated for the extract was 861.3 µg/ml, however, the inhibition was modest compared to that of acarbose (IC50, 16.8 µg/ml).
Table 5. α-Amylase inhibitory activity of C. cartilaginea extract and acarbose
|
Sample concentrations |
|
% of inhibition |
IC50 (µg/ml) |
|
C. cartilaginea extract (mg/ml) |
0.63 |
37.0 ± 0.2 |
|
|
|
1.3 |
66.0 ± 0.1 |
|
|
|
2.5 |
82.0 ± 0.0 |
|
|
|
5.0 |
100.0 ± 0.5 |
861.3 |
|
Acarbose (µg/ml) |
10 |
30.0 ± 1.2 |
|
|
|
20 |
60.0 ± 0.4 |
|
|
|
40 |
79.0 ± 0.8 |
|
|
|
80 |
100.0 ± 0.3 |
16.8 |
Diabetes and its complications constitute a major health challenge globally. Until now, there are no curative agents for diabetes [24]. The WHO has stressed the need for investigating and exploring natural antidiabetic agents such as those derived from plants. This is because traditional medicine usually comes with a better safety profile compared to synthetic medications [25].
In this work, the potential of C. cartilaginea leaf extract in managing diabetes was investigated by evaluating its anti-diabetic effect in rats and by determining its antioxidant activity as well as its ability to inhibit α-amylase in vitro. Alloxan was injected to induce diabetes mellitus in rats via intraperitoneal administration (200 mg/kg). Alloxan partially damages insulin-secreting beta cells in the pancreas. The resultant insulin deficiency may disrupt biological events that control blood glucose levels and regulate lipid homeostasis [26]. Degradation of β-cells by alloxan and the lack of insulin also causes a body weight decrease and may also be associated with polyphagia and polydipsia [27].
Indeed, our data showed a decrease in the weight of diabetes-induced rats. This drop in weight may be caused by the ensuing structural protein catabolism needed to produce cellular energy, a mechanism that cells utilize to make up for the diabetes-induced intra-cellular carbohydrate deficiency [28]. On day 14 of treatment with the 200 mg/kg C. cartilaginea leaf extract, a modest increase, albeit not significant, was noticed in the body weight of treated animals. The slight insignificant increase is probably due to the short duration of the observation period [21].
Following diabetes induction through alloxan administration, a marked elevation of fasting serum glucose level was noted in all investigated animal groups in comparison with the healthy control group 1, indicating successful diabetes induction. Interestingly, upon treatment with C. cartilaginea leaf extract (groups 3 and 4), there was also a significant reduction (P < 0.05-0.001) in blood sugar levels. The decrease in serum glucose was comparable to the one induced by glibenclamide in group 5. The pronounced decrease of serum sugar levels in C. cartilaginea extract suggests that the plant intrinsically possesses effective hypoglycemic constituents. One potential mechanism that explains the anti-diabetic effect is that the extract activates β-cells to synthesize and secrete insulin. It has been shown that a single intra-peritoneal alloxan shot at a dose of 170–200 mg/kg body weight appears to be most effective in inducing a diabetic state in rats, driven by alloxan-induced degradation of beta cells of the pancreas [26]. That leaves a portion of still intact β-cell that could be stimulated by agents or extracts to synthesize and release insulin.
Other possible mechanisms of action underlying the hypoglycemic effect of C. cartilaginea include sensitizing tissues to insulin, promoting the uptake of glucose by the liver and skeletal muscles, inhibiting hepatic gluconeogenesis, or slowing β-cell degeneration [29]. In corroboration with that, evidence from a previous study showed that C. spinose, a well-known Capparis species, exerts multiple hypoglycemic effects such as inducing the process of gluconeogenesis, stimulating glucose cellular uptake processes by skeletal muscles, and preventing degeneration of beta cells [30]. More mechanistic experiments are warranted to explore the exact pharmacology/mode of action of the plant.
This antidiabetic effect of C. cartilaginea leaf extract shown in the present work was time-dependent but was not dose-dependent. Unexpectedly, the lower dose of the plant extract (200 mg/kg) produces a more pronounced hypoglycemic effect compared to the higher dose (400 mg/kg). This could be caused by some other substances found in higher amounts in the concentrated plant extract, which may have antagonized the hypoglycemic activity of C. cartilaginea [31]. Another possibility is that a highly concentrated extract hinders the absorption of the bioactive ingredients across cellular membranes due to high viscosity [32]. In consistence with our findings, results from previous studies reported that lower doses of Piper longum and Bidens pilosa extracts showed greater hypoglycemic effects compared with the effects exhibited by the higher dose extracts [32, 33].
Hyperlipidemia is often a complication of diabetes mellitus that results from alterations in fat metabolism and storage [34]. Insulin deficiency appears to stimulate the release of free fatty acids from body fat storage sites into the systemic circulation [35]. Therefore, controlling plasma lipid levels and maintaining them at normal levels are goals when treating diabetic patients. In the present work, significant elevation in blood cholesterol, LCL, TG, and a reduction in HDL in diabetic untreated rats were recorded. The findings align with a previous work that reported an increase in serum sugar levels is often associated with an elevation of serum cholesterol, TG, and LDL and a reduction in HDL levels [36]. This alteration in serum lipids could increase the chances of developing ischemic heart diseases [37]. Interestingly, the 200 mg/kg C. cartilaginea leaf extract exerted a promising potential in restoring lipid levels. The extract reduced TC, TG, LDL and increased HDL in diabetic rats. The anti-hyperlipidemic effect of C. cartilaginea may be via potentiating the endogenous secretion of insulin, which in turn activates lipoprotein lipases to break down lipids [21]. Other possible mechanisms for the anti-hyperlipidemic effect may include inhibiting cholesterol absorption, sequestering bile secretions in the digestive system, and decreasing cholesterol biosynthesis within the liver. Furthermore, the extract might be enhancing the uptake of LDL by activating lecithin cholesterol acyl transferase (LCAT) which plays a role in lipid homeostasis. LCAT also aids in increasing HDL levels, which may explain how the cartilaginea extract raises HDL levels [35, 38]. The above potential hypolipidemic mechanisms for C. cartilaginea extract have been suggested for the hypolipidemic activity of Capparis spinosa buds extract, a well-known Capparis species [35]. The significant lipid-regulatory profile of C. cartilaginea may provide some protection against not only diabetes but also against cardiovascular diseases and may be of help in controlling obesity complications.
The hypoglycemic and hypolipidemic effects exerted by C. cartilaginea leaf extract are attributed to its bioactive constituents. The present study revealed that C. cartilaginea leaf contains alkaloids, carbohydrates, glycosides, saponins, diterpenes, flavonoids, anthraquinone glycosides, phenols, and tannins, however, work is needed to determine which of them is responsible for the plant pharmacological activity. The hypoglycemic effects of naturally occurring alkaloids have been reported. For instance, alkaloids isolated from medicinal plants like Catharanthus roseus and Ervatamia microphylla have exhibited antidiabetic effects in animal models [39, 40]. In addition to alkaloids, some physicians advise diabetic patients to consume flavonoid-containing dietary products. Rutin is a flavonoid that is found in several types of plants, that is believed to possess a significant antidiabetic effect by altering glycolysis and gluconeogenesis. Rutin also stimulates glucose uptake by tissues by activating insulin receptor kinases and insulin-dependent glucose transporters [41]. Moreover, rutin has shown a significant antioxidant reserve which may protect pancreatic beta cells from oxidative damage, thereby mitigating diabetes symptoms [35]. Since rutin has been reported as a bioactive ingredient of C. cartilaginea [10], it may be the active ingredient responsible for the glucose-lowering effect exhibited by C. cartilaginea. Saponins present in C. cartilaginea extract may be contributing to its anti-diabetic potential. For instance, saponins in ginseng were able to reverse the hyperglycemia exhibited by drug-induced as well as by genetically engineered diabetic rodents [42].
Controlling post-prandial blood sugar is a major therapeutic approach for the management of early-stage diabetes. This may be achieved by delaying or preventing carbohydrate digestion and glucose absorption within the gastrointestinal system. Indeed, inhibition of oligo-saccharide-hydrolyzing such as alpha-glucosidase reduced post-prandial glucose levels [43]. Indeed, multiple alpha-glucosidase inhibitors have been and still are employed in treating diabetes including acarbose [44]. In the present study, C. cartilaginea extract showed considerable α-amylase inhibitory effects when compared with acarbose, a reference drug. This suggests that C. cartilaginea may be utilized to prevent spiking of blood glucose after meals, particularly in diabetic patients.
Prolonged hyperglycemia raises oxidative stress in living systems and alters normal biological anti-oxidant mechanisms, thereby promoting lipid peroxidation and leading to vascular complications [45]. Also, an imbalance between ROS and biological antioxidant reserve may promote tissue insulin resistance [46]. In the present study, C. cartilaginea extract showed a promising antioxidant effect, as evidenced by the DPPH assay in vitro. Although this antioxidant activity was lower than that of the standard antioxidant vitamin C, it still possessed a significant proton-donating free radical scavenging activity that may add to its arsenal of antidiabetic effects. Further in vivo studies to determine the plant antioxidant effect on oxidative stress markers within hepatic and pancreatic tissues are warranted. Phenol-containing compounds are known as efficient hydrogen donors, which makes them good antioxidant agents [47]. The total phenolic content was determined in C. cartilaginea extract and the results indicate that C. cartilaginea extract is indeed rich in phenols (25.3 mg GAE/g dried extract).
CONCLUSION
In conclusion, the finding of this work supports the use of C. cartilaginea leaves for diabetes management which has been employed in folk medicine for decades. The study shows the ability of C. cartilaginea leaf extract to treat diabetic rats, a finding that has not been reported in the literature. Moreover, the administration of C. cartilaginea extract normalized multiple lipid parameters in blood. Therefore, the extract appears to hold promise in protection protocols against diabetes-associated vascular complications, and cardiovascular diseases and may prove helpful in obesity management. Also, C. cartilaginea leaf extract-induced enzymatic inhibition against α-amylase may be of use in the management of postprandial hyperglycemia. The combined free radical scavenging (antioxidant) and the anti-diabetic properties of C. cartilaginea underscores its potential in preventing diabetic-associated complications. Further mechanistic and clinical investigations are needed to assess the plant's therapeutic potential, pinpoint the mechanisms involved, and explore potential adverse effects.
ACKNOWLEDGMENTS : The authors thank the Faculty of Pharmacy, Sana’a University, Yemen for providing logistics to perform the experiments. Special thanks to the Yemen Drug Company for Industry & Commerce (YEDCO) and Sehatak Laboratories for Medical Analysis (Sana’a, Yemen) for the laboratory facilities provided.
CONFLICT OF INTEREST : None
FINANCIAL SUPPORT : None
ETHICS STATEMENT : The institutional animal ethical committee approved the protocol for the experiment (No. 15-2/8/2021).