
New Therapeutical Procedures of Peyronie’s Disease: Transfer Capacitive Resistive Energy in Association with Hydroelectrophoresis with Verapamil
Carlo Maretti 1*, Domenico Canale 2
1 Department of Andrology - CIRM Medical Center – Via Somaglia 10 - 29121 Piacenza, Italy.
2 University of Pisa Medical School and Hospitals, - Via Paradisa, 2 - 56124 Pisa, Italy.
*Email: carlomaretti @ tin.it
ABSTRACT
Introduction: Efficacy evaluation of a new treatment, improving the symptoms of Peyronie’s disease (PD) in patients with a curvature deformity < 30° and with an onset of symptoms of at least 6 months before the treatment. We investigated the effects of Transfer Capacitive Resistive Energy (TCARE) therapy accompanied by hydroelectrophoresis (HEP), a new electromotive system, for the transcutaneous delivery of Verapamil in men with PD. Materials and Methods: Sixty-one patients affected by PD were enrolled. They were randomly divided into two groups: Group 1 (n. 30 patients, median age 56, range 49-62 yrs) was assigned to receive only TCARE; Group 2 (n. 31 patients; median age 58, range 51-60 yrs) received both TCARE and HEP. Every patient underwent 16 treatment sessions, 2 sessions a week for each group. TCARE was performed with resistive energy and each treatment lasted 15 minutes. In Group 2 TCARE was also followed by HEP (with Hydro4and apparatus, Swiss4Med SA, Morbio Inferiore, Switzerland). HEP delivered 10 mg/4ml of Verapamil per session (2 ampoules of Verapamil 5mg/2ml each; Isoptin, BGP products, Rome, Italy) for a 20-minute lasting. The endpoints were: a pain increase in erection, the International Index of Erectile Function questionnaire (IIEF-15) scale score, and penile curvature (in degrees). They were evaluated at the beginning of the study, at the end and three months after the discontinuation of the treatment. The pain was measured by using the Numeric Rating Scale (NRS) for pain 1-10 and the erectile function by IIEF15. The penile curvature was measured instead by using photography, a personal paper protractor after injection of PGE1 10 mcg. Some side effects during or immediately after the treatment were recorded. Statistical analysis was performed using ANOVA for repeated measurements, corrected with Bonferroni. The side effects were compared between the two groups using the Chi-square Test (test χ2). Results: The pain, the erectile function, and the penile curvature were all significantly improved with both treatments (p<0.001). In Group 2 (TCARE + HEP) the improvement was greater than Group 1 (p<0.001 for IIEF and curvature; p <0.05 for pain). The amelioration was maintained until three months after the end of treatment. No relevant side effects were observed or indicated by the patients. Conclusions: TCARE followed by Verapamil administration by HEP is an effective and safe treatment for PD.
Key words: Peyronie's Disease (PD), medical therapy, Verapamil, Transfer Capacitive Resistive Energy (TCARE), Hydroelectrophoresis (HEP).
INTRODUCTION
Peyronie's disease (PD) is a rare situation concerning middle-aged men, causing the penis curvature. The magnitude of penile deformity is a critically important factor in Peyronie's disease as it is associated with increased difficulty in penetrative sexual intercourse and in turn with negative psychosocial consequences [1, 2]. The disease development is not well perceived. The subjects are men predisposed to genetic conditions (locally produced growth factors) or metabolic dysfunctions (diabetes, hypertension) [3]. The penile trauma causes inflammation in the tunica albuginea, provoking anomalous scars and the replacement of the normally elastic tissue with a hard nerve fiber. During the erection, this connective tissue does not “stretch”, provoking a curvature of the penis along the side of the “plaque” [4]. Unfortunately, a variety of deformities could be caused by these plaques. Pain and erectile dysfunction may be accompanying symptoms [5]. Originally, PD was regarded as a phenomenon, which spontaneously resolved itself; however, more recent studies have indicated that few or no patients experienced disease resolution, whereas, in a large majority of patients, the disease worsened [5, 6]. A third of men disturbed by PD have painful erections, while a smaller percentage of men with PD develops erectile dysfunction. Discomfort occurs during an erection when inflammation is associated with tissue injury [1]. Several patients with PD at an early stage can continue to have sexual activity, but those with a severe penile deformity have difficulty in sexual intercourses. The literature deals with ordinary and sometimes anecdotal benefits about the efficacy of conservative therapy in the initial phase with pain and inflammation [6]. Deformity magnitude also influences treatment choice when surgical correction is indicated [2]. The treatment with a Collagenase from Clostridium histolyticum (CCH) injected directly into the corpora cavernosa plaques, has recently been approved by FDA [7]. The reported side effects (penile hematomas and corpora ruptures) and the high costs, limit the use of such a treatment in patients with stable disease and a curvature > 30°. This means that a relatively large number of patients still require medical treatment other than CCH. Some surveys have suggested the positive results obtained from the intraplaque injections of Verapamil [8]. However, intraplaque injections are painful and provoke discomfort, and sometimes hematomas; moreover, the micro-trauma caused by the needle action may aggravate the disease [9]. These considerations have prompted us to test a new therapeutic approach to PD by employing TCARE therapy [10]. This is a non-invasive and painless treatment modality, well known in orthopedics and rehabilitation medicine; the energy transfer caused by the instrument has anti-inflammatory, analgesic, and restorative actions due to a local increase of endogenous temperature, vasodilation, and microcirculation [11]. In this trial, TCARE treatment has been associated with hydroelectrophoresis (HEP), which provokes a transcutaneous delivery of the therapeutic principle, Verapamil, in the area of the plaque [12, 13].
MATERIALS AND METHODS
This was a prospective multicenter study. All patients complaining of untreated PD were involved in the study. These patients were enrolled between 2nd October 2018 and 10th September 2019. PD was delineated by the presence of plaques in the penis tunica albuginea. PD was diagnosed thanks to medical history, physical examination, and basal and dynamic duplex scanning of the penis (i.e. after intracavernosal injection of Alprostadil [PGE1] 10 µg) [14]. The following laboratory assessments were carried out on each patient: Body Mass Index (BMI = weight in Kg/height in m2), blood pressure, complete blood count (CBC), liver enzymes, blood sugar, glycated hemoglobin, and Prostate Specific Antigen (PSA). The following appraisals were conducted before and after the treatment. Objective data on the nature and magnitude of the penile deviation were obtained during the above-mentioned ICI (intracavernosal injection of Alprostadil) procedure associated with the penile dynamic ultrasounds, on the basis of photo archives using the Kelami method [15] and calculated by us using a paper protractor to measure bendings on midsagittal and transverse planes [9]. The following parameters were estimated prior to therapy: pain on erection using a visual pain scale 1-10 [16], satisfaction with vaginal penetration according to the International Index of Erectile Dysfunction (IIEF) 15 scale score [17] and penile deviation in degrees (Figure 1). The same parameters were again evaluated 3 months after the end of the treatments. The acute and chronic side effects of the treatments were assessed as well.
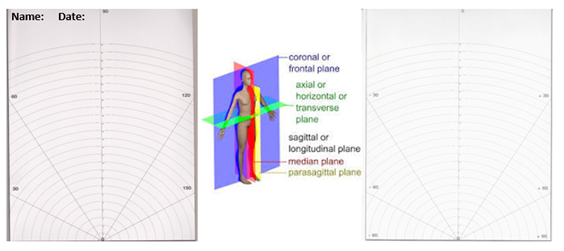
Figure 1 – A double-faced paper protractor with the patient’s name and date indications.
Bending can be measured with a protractor graduated from 0° to 180° degrees for the midsagittal plane and from -90° to +90° for the transverse plane.
Inclusion Criteria
All patients with a diagnosis of PD were considered candidates for the present study.
Exclusion Criteria
The exclusion criteria were as follows: refusal to participate in the study (12 cases), previous penile surgery or trauma (2 cases), pelvic surgery (6 cases), uncompensated diabetes/hypertension (13 cases), tobacco and/or alcohol abuse (12 cases), penile deviation > 30° (15 cases), and any previous treatment for PD (21 cases).
Patient Randomization
Randomization was carried out using an online randomizer: https://www.randomizer.org/. The patients were randomized into two groups: Group 1 receiving only TCARE, 2 sessions of 15 minutes each per week for 8 weeks, whereas Group 2 receiving TCARE + HEP Verapamil 10mg/4ml x 2 sessions of 20 minute each per week for 8 weeks. Blindness could not be guaranteed because the mixture gel+drug (see next paragraph) was immediately used after preparation, and the mixture was prepared by the researchers since no nurse was available.
TCARE
TCARE (or RC circuit or Resistance-Capacitor circuit) (Figure 2) consists of two plates (called armatures) placed one opposite the other and of an electric generator, which connected to the armatures, creates a difference in potential, which is translated into a positive charge (positive armature) and a negative charge (negative armature) and allows the movement of the electrolytes inside the tissues. The positive armature, containing an insulating material, attracts the negative electrical charges, while the negative armature attracts the positive ones (Figure 3). The movement of electrolytes generates an increase in temperature from inside, called "endogenous". It develops a cascade of beneficial reactions in the body that help speed up the recovery process. The biological effects produced by Tecartherapy are mainly an increase in the microcirculation and vasodilation, where the achievement of these effects depends on the amount of energy supplied by the TCARE device [10]. To obtain an increase in microcirculation, the operator must set the instrument to a low energy level (athermia). By increasing the energy level, vasodilation will be reached. The increase in microcirculation reduces the pain in the acute inflammatory phase with a major production of ATP and a major consumption of O2 by the affected cells [11]. The endogenous heat fosters vasodilation that, determining a blood volume rise, increases natural tissue repair processes and in particular tissue fibrosis, while the patient experiences a slight sensation of warmth in the treated area [18]. We adopted the resistive TCARE method with adjustable intensity of energy (around 8%). TCARE with its 0.5 MHz long wave radiofrequency is ideal for the damaged tissue treatment with high resistance to the passage of current (such as the albuginea of the penis).

Figure 2: a complete picture of TCARE [8].
TCARE is an electric generator to which two plates, respectively named positive and negative armature, are connected.
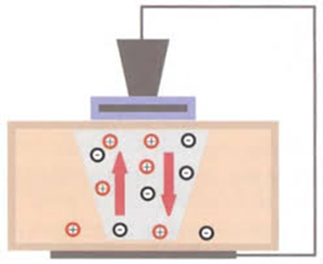
Figure 3: TCARE working. The positive armature attracts the negative electrical charges of the insulating material while the negative armature attracts the positive ones.
Hydroelectrophoresis technique (HEP)
Hydroelectrophoresis [12] is based on the use of pulsed electric currents to convey the active ingredients of drugs (liquid and/or powder) in a special gel (Hydro4Gel - Gel Fisio) formulated on purpose to keep them in suspension. The system schematically consists of a current generator, a particular dispenser with an electrode (the Roll-On dispenser), which polarizes one or more active ingredients and a passive electrode. The physical characteristics of the electric current are those of a one-way pulsed current, triangular in shape, with a sinusoidal pattern, with a variable frequency, which can carry the active principles to a depth, previously set in the device, that varies from a few millimeters to 10 centimeters without damaging the skin and eliminating all the complications of the injections. Thus, the membrane channels of the affected tissue are activated allowing the active principles to penetrate the cells [13]. The goal is to transport the active ingredients to the cell interstitium, increasing the bio-availability of the drug in the affected area and therefore improving its therapeutic action. Authors perform HEP using a Hydro4and apparatus (Swiss4Med SA, Morbio Inferiore, Switzerland) (Figure 4) and the content of 2 ampoules of Verapamil (Isoptin®, each ampoule containing 5 mg in 2ml, BGP Products, Rome-Italy) mixed in the dispenser, which contains 10 ml specific gel (hydro4gel™) so that the mixture hydro4gel+drug flows through the Roll-On dispenser. The HEP is set at the desired level and an operator rolls up and down the Roll-On dispenser on the flaccid penis in correspondence of the plaque for 20 minutes [19]. The procedure is repeated twice a week for 8 weeks.
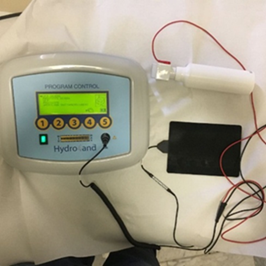
Figure 4: a complete picture of the Hydro4and apparatus (Swiss4Med SA, Morbio Inferiore, Switzerland). A white dispenser is attached to the special polarization chamber (Roll-On dispenser).
Endpoints and Statistical Analysis
With regard to the efficacy of the treatment, the endpoints were: pain grade, IIEF15 score, and penile curvature assessed using ultrasonography + ICI PGE1, 10 mcg., photography, and a personal paper protractor, which allowed to measure, the curvature angle with precision during various medical checks. The differences inside and between the groups were analyzed with ANOVA for repeated measures corrected by Bonferroni. The side effects were compared between the two groups using the Chi-square Test (test χ2).
RESULTS
Sixty-six patients were eligible for participation in the study: 32 patients were randomly allocated to Group 1 (only TCARE) and 34 patients to Group 2 (TCARE + HEP with Verapamil). Two patients of Group 1 and three patients of Group 2 dropped the study (protocol violation, transfer to other towns, or further reasons). So, 30 patients of Group 1 and 31 patients of Group 2 completed the study and were evaluated. Table 1 shows the clinical and demographic features of the patients. No significant difference was found between the two groups. Table 2 shows the results of the study concerning pain, IIEF 15 score, penile curvature, and side effects. There was a significant improvement for some parameters after each treatment (p<0.01). This increase was higher in Group 2 where TCARE was associated with HEP with Verapamil (p<0.05 for pain; p<0.01 for IIEF15 score and penile curvature). The side effects were mild and negligible (transient hypotension in two patients). One of the most significant effects was certainly the improvement of the penile curvature (<0.01) both detected through the photography and the paper protractor. In Group 1 (TCARE) the improvement was about 5 degrees while in Group 2 (TCARE +HEP with Verapamil) it was about 9 degrees (<0.01). These data were confirmed after three months from the end of the treatments through the same endpoints. Pain is another standard, which was improved effectively (<0,05) after two treatments and in any case, it decreased mainly in Group 2. Each patient was very satisfied with the results.
Table 1: Baseline demographic and clinical characteristics for each group participating in the study. Group 1: patients treated with TCARE alone. Group 2: patients treated with TCARE + HEP (details in the text). Data are shown as median values, ranges in parentheses. No significant difference was observed.
|
|
Group 1 30 patients |
Group 2 31 patients |
P-value |
|
Age in years |
56 (49-62) |
58 (51-56) |
0.345 |
|
Body mass index (BMI) in Kg/m2. |
24 (20-28) |
23.5 (20-27) |
0.310 |
|
Compensated hypertension (%) |
12 (40%) |
11 (35.5%) |
0.207 |
|
Dupuytren’s contracture (%) |
0 |
0 |
Not tested |
|
Compensated diabetes (%) |
6 (20%) |
7 (22.6%) |
0.434 |
Table 2: Comparisons between the pain score on erection (NRS, Numeric Rating Scale for Pain of 1-10), International Index of Erectile Function (IIEF15) scale score, penile deviation in degrees, assessed at the beginning of the study, in the end, and 3 months after TCARE in Group 1 or TCARE associated with HEP administration of Verapamil in Group 2 (2 sessions weekly for 8 weeks in both Groups; details in the text).
|
Administration |
Group 1 30 patients treated with TCARE alone |
Group 2 31 patients treated with TCARE + HPE |
P-value (ANOVA) |
||||||
|
BEFORE (a) |
END (b) |
AFTER (3months) (c) |
BEFORE (d) |
END (e) |
AFTER (3months) (f) |
(a) vs (b) and (c) (d) vs (e) and (f) |
(b) vs (c) Group A vs (e) vs (f) Group B |
||
|
Pain score |
3.3±0.19 (2-6) |
2.23±0.12 (0-3) |
1.82±0.11 (0-2) |
3.54±0.16 (1-5) |
0.87±0.12 (0-2) |
0.74±0.11 (0-2) |
<0.001 |
NS |
<0.05 |
|
IIEF 15 scale score |
24.62±0.39 (21-29) |
26.43±0.30 (24-29) |
26.56±0.25 (24-29) |
24.32±0.30 (21-29) |
27.80±0.19 (27-30) |
27.83±0.18 (27-30) |
<0,001 |
NS |
<0.01 |
|
Penile deviation (degrees) |
17.8±1.01 (10-25) |
13.1±0.77 (5-20) |
12.7±0.77 (5-20) |
17.8±1.0 (10-26) |
9.7±0.81 (0-10) |
9.4±0.76 (0-10) |
<0,001 |
NS |
<0.01 |
|
Side effects (%) (Test χ2) |
2/30* (6.7%) |
0/31 (0%) |
|
||||||
Data are shown as median values±SE, ranges in parentheses. Statistical analysis was performed using ANOVA for repeated measurements corrected by Bonferroni. The side effects were recorded as well and were compared using the Chi-square test (Test χ2).
Keys: * two patients had mild hypotension
CONCLUSIONS
Our data show that the delivery of Verapamil, obtained by HEP and preceded by TCARE in the penile areas affected by fibrosis, can treat symptoms such as pain and structural changes, penile curvature, and plaque extension.
TCARE has been already used in a variety of clinical conditions, mainly in orthopedics and physiotherapy, for its analgesic, anti-inflammatory, and restorative actions induced by the local increase in microcirculation, temperature, and vasodilation. These actions provoke a reduction of the inflammatory condition typical of PD and its painful symptoms. The increase in microcirculation reduces pain in the acute inflammatory phase with a major production of ATP and a major consumption of O2 by the affected cells. The endogenous heat fosters vasodilation that leads to increase blood volume, natural tissue repair processes, and particularly tissue fibrosis, while the patient experiences a slight sensation of warmth in the treated area [20-22].
Verapamil has been widely studied and used in the treatment of PD [23, 24]. One of the major limits of these studies is the delivery of the drug by intralesional injection. This procedure itself provokes a further induction of micro-scars that are considered the primum movens of PD. The action of Verapamil is to block voltage-dependent calcium channels, by relaxing the tone of the smooth muscle and, thus, dilating the blood vessels. Calcium antagonists have been found to reduce extracellular matrix production, induce procollagenase synthesis, and inhibit interleukin-6, vascular endothelial growth factor, and proliferation of fibroblasts [25]. For these actions, it has also been used in the treatment of hypertrophic scars and keloids [26]. Thanks to the use of HPE, the negative effects of injections have been canceled.
We hypothesize that the preliminary treatment with TCARE, which increases microcirculation, vasodilation, and endogenous heat, further enhances the actions of Verapamil on the tunica albuginea and the cavernosal tissue. This occurs thanks to HEP without the deleterious effect of injections.
Limits of the study are represented by the absence of a placebo. However, the intralesional administration of a saline solution has been shown to have an active effect on the plaque.
Pain and sexual function were assessed by administering a validated questionnaire to patients; therefore, the results of the therapies were evaluated by the patients themselves. Further assessments of plaque and penis deformities were conducted using objective methods (ultrasonography + ICI PGE1, 10 mcg., photography, and personal paper protractors, which allowed to measure, the curvature angle with precision) in order to minimize the authors' influence as much as possible.
In conclusion, hydroelectrophoresis performed with a Hydro4and apparatus, associated with TCARE is a safe and effective method of administering intracavernous drugs to relieve the symptoms of PD and significantly reduce plaque and penile curvature. Further studies are necessary to increase the number of samples and define the clusters of patients that can benefit from the treatments.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
REFERENCES

