Investigating Semaglutide in Adult Patients on Body Weight Compared with Other GLP-1 Drugs
Shroug Farrash1, Lujain Aleisa1, Nardeen Alhazmi1, Nouf Almatrafi1, Taef Alharbi1, Shahad Kelantan1, Lina Alotaibi1, Wed Hunaydi1, Sara Alnimari1, Noor Alqarni1, Einaf Babtain1, Hanadi Bazuhair1, Yosra Alhindi2*
1Faculty of Pharmacy, Umm Al-Qura University, Makkah, KSA.
2Department of Pharmacology and Toxicology, Faculty of Medicine, Umm Al-Qura University, Makkah, KSA.
*Email: [email protected]
ABSTRACT
Obesity and diabetes, one of the most common diseases can cause a several complications. In diabetic patient with type 2 we mainly use an oral medication with varies mechanism of action such as: GLP-1 medication. To look at semaglutide's (a new glucagon-like peptide receptor agonist; GLP-1 RA) effectiveness in treating individuals with diabetes and obesity. We followed the guidelines of the PRISMA checklist for conducting this study. On 23rd October 2022, we run a systematic search ““semaglutide”, “GLP1”, ''diabetes type 2'', ''obese'' and ''HBA1C''” in five databases named: Scopus, Google Scholar, PubMed, Virtual Health Library and Web of Science. We included 18 papers. Subcutaneous semaglutide was used in ten placebo-controlled and seven active-controlled trials, including nine hundred fifty-five participants. We were only able to locate one oral semaglutide experiment. When compared to a placebo, subcutaneous semaglutide 0.5 and 1 mg reduced HbA1c by 1.01% (95% CI 0.56 to 1.47, I2=93%) and 1.38% (1.05 to 1.70, I2=90%), respectively. The glycemic effectiveness of both dosages was superior to that of other antidiabetic drugs such as insulin glargine, liraglutide, dulaglutide, sitagliptin, and exenatide.
Systolic blood pressure, hemoglobin A1c, and body weight are all significantly reduced by semaglutide, a potent once-weekly GLP-1 RA. Nonetheless, there is a higher likelihood of gastrointestinal side effects with it. Results regarding pancreatitis and retinopathy should be evaluated in further post-approval pharmacovigilance studies and interpreted cautiously.
Key words: Semaglutide, GLP-1, Diabetes, Body weight, Obese
INTRODUCTION
Obesity is one of the most popular diseases, it’s a complex disorder involving excessive amount of fat and lipid in body that can cause many of diseases, Obesity is one of the most popular diseases, it’s a complex disorder involving excessive amount of fat and lipid in body that can cause many of diseases [1]. There are multiple mechanisms that are involved in the pathogenesis of obesity such as high caloric intake, genetic factors, lack of activity and exercise all can lead to obesity progression [1, 2].
Obesity can lead to several medical conditions and complications such as cardiovascular diseases, infertility, cancers, insulin resistance which may lead to type 2 diabetes. Diabetes is a broad category of metabolic disorders that are defined by blood glucose levels that are out of control because of either inadequate insulin production or insulin resistance. There are several indications and symptoms associated with diabetes, such as increased appetite, thirst, and fatigue [3, 4].
Diabetes has three main types, Type 1 (IDDM): Usually the body’s attack its own self and destroys the insulin producing cells in the pancreas (islet of Langerhans) and it’s usually diagnosed in children. Type 2 (NIDDM): About 90% of patient with diabetes have type 2. It occurs when body cells become resistant to the action of insulin hormone and the pancreas can’t afford much more insulin to overcome this resistance. Gestational diabetes: It accuses during pregnancy at any trimester but more in the second or third trimester. It’s usually disappeared after giving birth [5, 6].
Hyperglycemia and a number of associated metabolic problems are hallmarks of diabetes mellitus, a chronic illness. High rates of death and morbidity have been linked to both the disease's inherent burden and inadequate glycemic management. The Centers for Disease Control and Prevention (CDC) estimate that 34.2 million adults in the US have diabetes, and that number is rising.
According to reports, if preventative steps are not followed, half of Saudi Arabia's population will have diabetes by 2030. Furthermore, diabetes in Saudi Arabia has been referred to as an "epidemic" issue in a number of studies [5, 6].
The treatment of diabetic patients or patients who are at risk for diabetes should always start with non-pharmacological ways such as lifestyle modification [7]. Moreover, the pharmacological medications are usually added for a better outcome. Sulfonylureas is the most widely used class, but usually patients will require the addition of another medication from another class [7, 8].
Metformin is a biguanide agent that increases the insulin sensitivity and decrease the blood glucose, it can be used as monotherapy or in combination with other drugs. Thiazolidinediones increase the insulin sensitivity, but they are not favorable due to their high risk for CHF, bladder cancer, and bone fractures [7]. DPP-4 inhibitors also reduce the blood glucose level, but they have lower effect than other medications. Finally, we have GLP-1 receptor agonists which we will be focusing on [8].
Glucagon-like peptide-1 agonists are a class of medications used for the treatment of type 2 diabetes and obesity by working on the incretin system. Examples of drugs in this class including exenatide, liraglutide, dulaglutide, albiglutide, lixisenatide, and semaglutide, which we will focus on in this research [9]. 50% of the stimulation of insulin secretion following an oral glucose load is attributed to the incretin hormones GLP-1 and glucose-dependent insulinotropic polypeptide (GIP), which are inactivated by dipeptidyl peptidase-4 (DPP-4). This mechanism may become muted or, in certain situations, nonexistent in type 2 diabetes. However, the function of excreting insulin can be restored by administering pharmaceutical amounts of GLP-1. The benefits of this form of therapy include decreased glucagon production if blood sugar levels are high, increased insulin secretion, and delayed gastric emptying, thus, food intake is decreased, that is why can use it to treat obesity. Also, GLP-1 receptor agonists can promote β-cell proliferation while reducing their apoptosis [9, 10].
Due to the natural GLP-1's short half-life and fast inactivation by the enzyme DPP-4, long-acting GLP-1 receptor agonists provide superior glycemic control than their short-acting equivalents [9]. GLP-1 receptor agonists have been examined for their impact on weight reduction in people with and without diabetes. These medicines help patients lose weight by encouraging satiety and delaying stomach emptying. They can be used as supplements for lifestyle changes for weight control. The first GLP-1 receptor agonist to receive FDA approval for long-term weight control was the liraglutide product Saxenda, which was authorized in December 2014. The second GLP-1 receptor agonist to receive FDA approval for weight management was semaglutide, a 2.4 mg once-weekly injection, which was approved in June 2021. Additionally, the results of clinical trials assessing the impact of GLP-1 receptor agonist therapy on body mass index and weight loss showed better results than those obtained with the use of other antiobesity medications, and GLP-1 receptor agonists as a class have a better safety profile than the other antiobesity medications [11, 12].
MATERIALS AND METHODS
We searched extensive electronic databases and grey literature sources for random controlled trials comparing semaglutide to a placebo or other GLP-1 drugs. The main result was a shift in weight from baseline. The secondary objectives were variations in HBA1C, blood pressure, heart rate, and the frequency of hypoglycemia, as well as adverse effects on the gastrointestinal tract, pancreatitis, and diabetic retinopathy. These systematic reviews and meta-analyses are in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) declaration. Every study project followed a procedure that was entered into the FIGSHARE database.
Data sources
We used PubMed to search Medline, Ovid to search Embase, and the Cochrane Library. The keywords "semaglutide," "GLP1," "diabetes type 2," "obese," and "HBA1C" were among those we used in our search approach.
Study selection
Results for at least one of the predetermined outcomes of interest were available from randomized controlled trials (RCTs) that compared semaglutide, either subcutaneously or orally, with placebo or any other GLP1 medication in adult patients with type 2 diabetes (T2DM). The trials had to be completed for at least 12 weeks. The two separate reviewers evaluated all records at the title and abstract levels before looking at potentially eligible records in full text. A senior reviewer with experience in T2DM addressed any disputes between the reviewers.
Data extraction
A pre-designed extraction form was used by two reviewers to separately abstract data from eligible studies; a third reviewer arbitrated any disputes. To optimize the output of information when there were many reports for the same research, all accessible data were compiled. We retrieved data, ideally from published reports, in the event that study reports contained contradicting information. While we did not predefine particular dosages of interest for oral semaglutide since no dose has yet been authorized by the FDA or EMA, we retrieved data for subcutaneous semaglutide based on the prescribed doses (0.5 mg and 1 mg) or the closest comparable dose that was available. Our primary result was a change in body weight (BW) from baseline; changes in HbA1c, heart rate (HR), and the diastolic and distolic blood pressures (SBP and DBP, respectively) were secondary efficacy outcomes. Additionally, we retrieved data on the number of patients who had experienced any hypoglycemia, severe hypoglycemia, vomiting, or diarrhea at least once. Additional safety findings were prompted by worries that semaglutide or GLP-1s may be connected to acute pancreatitis and diabetic retinopathy. The criteria used in each research were utilized to collect data regarding safety outcomes.
Risk of bias assessment
Two independent reviewers evaluated the risk of bias within trials for the primary outcome using the revised Cochrane Collaboration's Risk of Bias Tool (R\B) version 2.0 [13]. Any disagreements were resolved by agreement. The overall bias risk of each qualifying study was graded as low in cases where the bias risk was low across all component domains, high in cases where the bias risk was high in at least one domain, and at some concern in other cases. Finally, we looked for small study effects that could indicate publication bias for the main outcome (change from baseline in body weight) in order to evaluate the likelihood of bias across studies using the Egger's test and visual examination of a funnel plot.
Ethical review
Since this study doesn't use any human subjects or private information, it doesn't need ethical review or permission.
RESULTS AND DISCUSSION
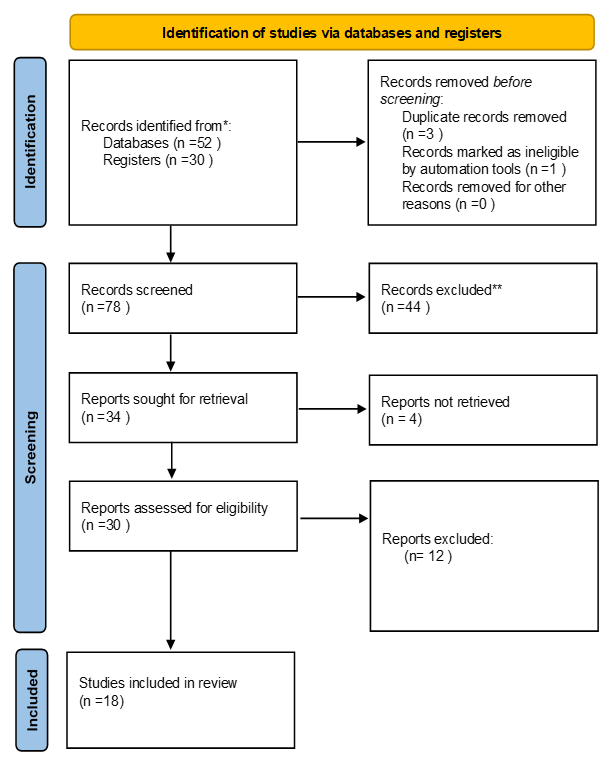
Findings from the Search and Study Features Figure 1 shows the outcomes of the study selection process. Our systematic review comprised 18 studies (9501 patients), including a post-hoc trial that was published while this publication was being prepared [7, 12, 14-21]. A summary of study characteristics may be found in Table 1. A placebo or another diabetes medicine was compared with subcutaneous semaglutide in ten trials [7, 18, 22-27] and seven studies [13, 28-32], respectively; in one trial, subcutaneous and oral semaglutide were compared with placebo [18]. Even though the remaining trials involved patients on either single [26] or dual [7-9, 23-25, 27] antidiabetic medication, two studies [28, 33] enrolled patients who had never had treatment. Semaglutide applied subcutaneously was used in one experiment [34].
|
|
|
Figure 1. PRISMA flow diagram |
Table 1. Major study characteristics
|
Mean body weight, kg |
Mean age, years |
Mean diabetes duration, years |
Mean HbA1c, % |
Patients randomised, n |
Study arms |
Background therapy |
Study duration, weeks |
Study ID |
|
A35.7 ± 6.3 |
55.3±10.6 |
8.6±6.2 |
8.2 8.2 7.9 |
1210 |
Semaglutide 2·4 mg (n=404) Semaglutide 1·0 mg (n=403) Placebo (n=403) |
MET ± (SGLT2i, or glitazone or SU) |
68 |
Davies et al. (2021) (STEP2) |
|
89·6 93·8 |
57·5 56·6 |
9·8 9·6 |
8·0 8·1 |
302 |
Semaglutide 1·0 mg OW(n=151) Placebo (n=151) |
SGLT2i ± (MET or SU) |
30 |
Zinman et al. (2019) (SUSTAIN 9) NCT03086330 |
|
96.2 95.4 |
56.4 56.7 |
9 9.4 |
8.4 8.3 |
809 |
semaglutide 1mg QW (n=404) exenatide ER 2mg QW (n=405) |
MET ± (SU or TZD) |
56 |
Ahmann et al. (2016) (SUSTAIN 3) NCT01885208 |
|
86.9 ± 21.0 89.0 ± 21.8 88.1 ± 22.1 88.6 ± 23.4 88.1 ± 22.1 |
55 ± 11 56 ± 11 54 ± 11 54 ± 11 |
3.8 ± 5.3 3.6 ± 5.1 3.4 ± 4.4 3.4 ± 4.6 |
7.9 ± 0.7 8.0 ± 0.6 8.0 ± 0.7 7.9 ± 0.7 |
703 |
Oral semaglutide 3 mg (n = 175) Oral semaglutide 7 mg (n = 175) Oral semaglutide 14mg (n = 175) Placebo (n = 178) |
None |
26 |
Aroda et al. (2019) (PIONEER) NCT02906930 |
|
91.0±21.4 90.8±21.0 |
66±7 66±7 |
14.7±8.5 15.1±8.5 |
8.2±1.6 8.2±1.6 |
3183 |
Oral Semaglutide (N=1591) Placebo (N=1592) |
Glucose-lowering and cardiovascular medication |
68 |
Husain et al. (2019) (PIONEER 6) NCT02692716 |
|
90.6 89.8 |
55.7 57.5 |
7.5 7.2 |
8.3 8.2 |
788 |
Semaglutide 1 mg OW (n=394) Canagliflizon 300 mg OD (n=394) |
MET |
52 |
Lingvay et al. (2019) (SUSTAIN 9) |
|
88.8 93.8 |
56.8 58.9 |
5.6 6.7 |
7.8 8 |
99 |
semaglutide 1mg QW (n=48) placebo(n=51) |
MET |
26 |
Davies et al. (2017) NCT01923181 |
|
91.1 91.3 |
57 58 |
7.2 7.7 |
8.1 8.1 |
821 |
Oral semaglutide 14 mg/w (n=411) Oral Empagliflozin 25 mg/d (n=410) |
MET |
52 |
Roadvard et al. (2020) (PIONEER 2) |
|
89.9 89.2 89.3 |
54.8 56 54.6 |
6.4 6.7 6.6 |
8 8 8.2 |
409 409 407 |
semaglutide 0.5mg QW semaglutide 1mg QW sitagliptin 100mg QD |
MET ± TZD |
56 |
Ahren et al. (2017) (SUSTAIN 2) NCT01930188 |
|
93.7 94 92.6 |
56.5 56.7 56.2 |
7.8 9.3 8.6 |
8.1 8.3 8.1 |
362 360 360 |
semaglutide 0.5mg QW semaglutide 1mg QW insulin glargine QD |
MET ± SU |
30 |
Aroda et al. (2017) (SUSTAIN 4) NCT02128932 |
|
71 71.7 72.2 |
58 58.7 59.2 |
8.1 9.4 9.3 |
8 8.1 8.1 |
239 241 120 |
semaglutide 1mg QW semaglutide 0.5mg QW other OAD |
SU or GLI or AGI or TZD |
56 |
Kaku et al. (2018) |
|
93.2 90 |
56 57 |
8.3 8.7 |
7.3 7.3 |
37 38 |
semaglutide 1mg QW placebo QW |
MET |
12 |
Kapitza et al. (2017) NCT02212067 |
|
91.8 92.9 91.8 91.9 |
64.6 64.7 64.8 64.4 |
14.3 14.1 14 13.2 |
8.7 8.7 8.7 8.7 |
826 822 824 825 |
semaglutide 0.5mg QW semaglutide 1mg QW placebo 0.5mg QW placebo 1mg QW |
< 2 OADs ± (BI or PRI) |
104 |
Marso et al. (2017) (SUSTAIN 6) NCT01720446 |
|
87 85.5 90.5 90.5 87.2 |
53.8 55.9 55.3 54.8 54.3 |
2 2.6 2.4 3.3 2.5 |
8.1 8 8.1 8 8.1 |
48 43 46 45 50 |
semaglutide 0.4mg QW semaglutide 0.8mg QW placebo QW liraglutide 1.2mg QD liraglutide 1.8mg QD |
MET |
12 |
Nauck et al. (2016) NCT00696657 |
|
96.4 95.5 95.6 93.4 |
56 55 55 56 |
7.7 7.3 7 7.6 |
8.3 8.2 8.3 8.2 |
301 300 299 299 |
semaglutide 0.5mg QW semaglutide 1mg QW dulaglutide 0.75mg QW dulaglutide 1.5mg QW |
MET |
40 |
Pratley et al. (2018) (SUSTAIN 7) NCT02648204 |
|
92.7 92.5 89.9 |
59.5 58.8 58.1 |
12.9 13.7 13.3 |
8.4 8.3 8.4 |
132 131 133 |
semaglutide 0.5mg QW semaglutide 1mg QW placebo QW |
BI ± MET |
30 |
Rodbard et al. (2016) (SUSTAIN 5) NCT02305381 |
|
70.8 69.4 |
58.8 58.1 57.9 |
8 7.8 8.1 |
8.2 8 8.2 |
103 102 103 |
semaglutide 0.5mg QW semaglutide 1mg QW sitagliptin 100mg QD |
None |
30 |
Seino et al. (2017) NCT02254291 |
|
89.4 96.9 89.1 |
54.6 52.7 53.9 |
4.9 3.6 4.1 |
8.1 8.1 8 |
128 130 129 |
semaglutide 0.5mg QW semaglutide 1mg QW placebo QW |
None |
30 |
Sorli et al. (2017) (SUSTAIN 1) NCT02054897 |
*Abbreviations: HbA1c, glycated haemoglobin; NCT number, clinicaltrials.gov identifier [35]; MET, metformin; SU, sulfonylurea; TZD, thiazolidinedione; GLI, glinide; AGI, a- Glycosidase inhibitor; OAD, oral antidiabetic drug; BI, basal insulin; PRI, premixed insulin; ER, extended release; QW, once weekly; QD, once daily; DPP4i, Dipeptidyl Peptidase IV inhibitor
Bias Assessment Risk Table 2 presents an assessment of the risk of bias. Eight studies [7, 23-26, 28, 33, 34] were found to have low risk of bias within the trials, while two studies [18, 25] had high risk of bias, primarily because of missing outcome data. In addition, one study raised some issues since it lacked details on the randomization procedure [27], and another study [33] was excluded from our assessment of bias risk since it lacked data related to our main outcome. The limited number of retrieved studies (seven for an active comparator and six for a placebo) made it impossible to use a funnel diagram or Egger's test to evaluate the small study impact [36].
Table 2. Overall Risk of bias (ROB2.0) for primary outcome
|
Study ID |
Randomization process |
Deviations from intended interventions |
Mising outcome data |
Measurement of the outcome |
Selection of the reported result |
Overall Bias |
|
Study 1 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 2 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 3 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 4 |
Low |
High |
High |
Low |
Low |
High |
|
Study 5 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 6 |
Unavailable data for primary outcome of interest |
|||||
|
Study 7 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 8 |
Low |
Low |
High |
Low |
Low |
High |
|
Study 9 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 10 |
Some concerns |
Low |
Low |
Low |
Low |
Some concerns |
|
Study 11 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 12 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 13 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 14 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 15 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 16 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 17 |
Low |
Low |
Low |
Low |
Low |
Low |
|
Study 18 |
Low |
Low |
Low |
Low |
Low |
Low |
An overview of the results We looked at the effectiveness and safety of semaglutide, a newly authorized GLP-1 RA, in this systematic review. We only synthesized data for subcutaneous, once-weekly semaglutide because there was just one trial that produced findings for oral semaglutide. Comparing semaglutide 0.5 and 1 mg to a placebo, the HbA1c was lowered by about 1 and 1.5%, respectively, without raising the risk of hypoglycemia. Moreover, semaglutide outperformed other GLP-1 RAs, insulin glargine, and sitagliptin in terms of effectiveness. Both dosages decreased body weight when compared to a placebo; moreover, semaglutide 1 mg decreased body weight when compared to other GLP-1 RAs, such as exenatide ER, liraglutide, and dulaglutide.
Additionally, semaglutide reduced systolic blood pressure while slightly increasing heart rate. Semaglutide medication was linked, in terms of safety outcomes, to a higher frequency of gastrointestinal side events but not to severe pancreatitis or diabetic retinopathy. On the other hand, data regarding pancreatitis and retinas should be interpreted cautiously because of potential underreporting and the absence of a standardization of these outcomes across all pertinent research. Advantages and disadvantages A recent isolated, industry-funded network meta-analysis supports our findings by revealing that semaglutide is more effective than other GLP-1 RAs at lowering body weight and HbA1c while having a similar risk of side effects [37].
In a similar vein, a pooled analysis supported by industry compiled the available data from a portion of the SUSTAIN studies [38-45]. Our work's strengths stem from our thorough bibliographic search, which included sources from the grey literature. We also assessed a number of outcomes that are considered significant in determining the best course of action when choosing between GLP-1 RAs and other antidiabetic medications, including the incidence of severe pancreatitis and diabetic retinopathy. In addition, we performed a sensitivity analysis for the primary outcome, incorporating only trials with a minimal risk of bias, and we evaluated the methodological quality of eligible studies using a stringent methodological methodology [13]. Our findings provide light on the drug's dose-dependent effects on lowering body weight and HbA1c using independent evaluations of the approved semaglutide dosages (0.5 and 1 mg).
In conclusion, our results are more clinically significant when compared to other GLP-1 RAs like dulaglutide, liraglutide, and exenatide ER, based on subgroup comparisons [23, 26, 40]. But, in evaluating our results, some restrictions must be considered. Even though there was increasing heterogeneity in the analysis for body weight and HbA1c, only heterogeneity for body weight was decreased when one trial with lower semaglutide dosages was eliminated. The study's findings or the participants' initial characteristics may provide an explanation. Specifically, when compared to the remaining trials, the period of the SUSTAIN-6 trials [7] was much longer and provided most of the data in most analyses. Furthermore, two studies only included Asian participants, which may also be a cause of variability [38, 41].
Furthermore, it's unclear if definitions for diabetic retinopathy and acute pancreatitis were the same across relevant research. In conclusion, our results are more clinically significant when compared to other GLP-1 RAs like dulaglutide, liraglutide, and exenatide ER, based on subgroup comparisons [23, 26, 40]. But, in evaluating our results, some restrictions must be considered. While increasing heterogeneity was seen in the analysis for both body weight and HbA1c, only body weight heterogeneity was decreased when one experiment using lower semaglutide dosages was eliminated.
CONCLUSION
Subcutaneous semaglutide applied once a week is effective in reducing systolic blood pressure, body weight, and HbA1c when compared to placebo and other antidiabetic medications, such as multiple different GLP-1 RAs. It is linked to a higher frequency of gastrointestinal adverse events, while post-approval pharmacovigilance studies are needed to investigate its connection to outcomes related to diabetic retinopathy.
ACKNOWLEDGMENTS : None
CONFLICT OF INTEREST : None
FINANCIAL SUPPORT : None
ETHICS STATEMENT : None