Creatine is a naturally occurring compound found in muscles that play a vital role in energy metabolism. It has been shown to have beneficial effects on skeletal muscle function and exercise performance, but recent studies have explored its potential role in various fields of medicine. The study aimed to analyze the accessible literature and illustrate the current state of knowledge regarding the use of creatine in these settings, as well as make predictions for further research. The association between low creatine concentrations and poorer mental well-being has been proven in the central nervous system. After many studies and insightful conclusions about the molecular mechanisms of creatine's action in the brain and the finding that it acts as a neurotransmitter, creatine began to be successfully studied as an antidepressant - both in monotherapy and as an adjunct to treatment with SSRI drugs. Years of research have shown that creatine acts through various and not fully understood mechanisms in the course and recovery of stroke. The use of creatine as an additional therapy in stroke prevention for high-risk groups and rehabilitation of stroke patients seems possible shortly. One of the most important aspects of chronic heart failure is the metabolic dysfunction that occurs in cardiomyocytes, including the impairment of the CR/PCR/ATP shuttle. Several studies investigating the role of creatine supplementation in patients with cardiovascular diseases have presented different findings. Therefore, creatine appears as a promising substance with supportive effects in the above-mentioned conditions; however, further research is needed to confirm that the benefit outweighs the risks.
INTRODUCTION
Creatine is a compound that can be found naturally in the body. The muscles hold 95% of its stores, with smaller amounts also present in the liver, kidneys, brain, and testes. It can be obtained from a typical omnivorous diet at a rate of approximately 1 gram per day since it is found in various foods, including red meat and seafood [1]. People who follow different kinds of vegetarian diets consume less of this substance because it is almost solely found in animal products. Therefore, their serum and muscle creatine levels are lower than those of omnivores [2]. Throughout recent years, creatine has become one of the most extensively researched and commonly used supplements, with a prevalence of supplementation ranging from 15-40% among athletes and military personnel, as it was found to improve athletic performance and increase muscle mass [1, 3].
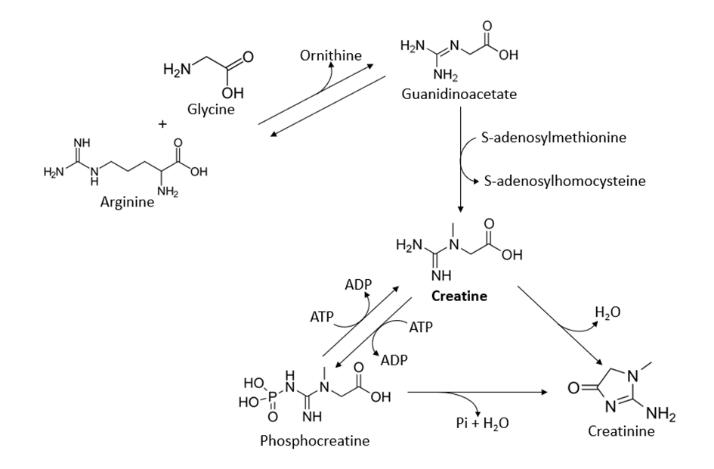
It is a nitrogenous compound, that the body produces from the amino acids glycine, arginine, and S-adenosylmethionine as the methyl donor. It is classified as a non-protein amino acid and its production occurs primarily in the liver and kidneys, but it can also be synthesized in the pancreas, testes, and brain to a lesser level [4]. It is stored in the body in two different forms: 40% is kept as free creatine, while 60% is phosphorylated to create phosphocreatine, which works by giving the body an additional source of energy through increased ATP production, especially during high-intensity exercise [1]. When ATP is used, it breaks down into adenosine diphosphate (ADP). Phosphocreatine helps to regenerate ATP from ADP by donating a phosphate group [1, 3]. The pathway of creatine synthesis involves several steps, as shown in Figure 1.
|
|
|
Figure 1. Pathway of creatine synthesis based on Kreider et al. [3] |
There is a significant body of research supporting the use of creatine as a supplement to improve athletic performance. Studies have shown that creatine supplementation can lead to significant increases in muscle strength and power, particularly in high-intensity exercise and activities that involve short bursts of energy, such as sprinting and weightlifting. It was also shown to increase muscle mass and size by enhancing protein synthesis, which can be beneficial for bodybuilders [5]. Moreover, some research suggests that creatine supplementation may support muscle recovery after exercise by reducing muscle damage and inflammation [3, 6]. The process of ATP regeneration can help to reduce muscle acidosis by decreasing the amount of acid produced in the muscles during exercise. In addition, creatine may help to buffer the synthesized acid, which can help to reduce the negative effects of acidosis on physical performance [5].
In addition to its use in sports, creatine may also have potential utility for a variety of medical conditions. In recent years, there has been growing interest in the usage of this substance in fields such as neurology, cardiology, psychiatry, and geriatrics [1]. We examine these non-sport applications, their workings, and their effectiveness in our evaluation, weighing whether the possible advantages outweigh the risks.
RESULTS AND DISCUSSION
Characteristics of creatine supplementation
Several dosing regimens have been investigated to understand how they impact creatine stores and the resulting performance benefits. Typically, the dosing protocol consists of two parts: the loading and maintenance phases. During the loading phase, a higher dosage of creatine is taken for a short period, usually 5-7 days, to rapidly saturate the muscle creatine stores. The typical dosage during the loading phase is 20-25 grams per day, divided into smaller doses taken throughout the day. Afterward, the dosage is usually reduced to 3-5 grams per day to maintain muscle creatine stores [3, 5]. After cessation of the supplementation, they usually return to the baseline within 4-6 weeks [3]. There is some debate about the necessity of implementing the loading phase. While it was shown to quickly increase muscle creatine stores by 20-40% [5], a study conducted by Hultman et al. [7] depicted that dosages characteristic for both loading and maintenance phases provide similar increase, but the effect in the group taking smaller doses is more gradual. Therefore, the dosing regimen should be adjusted depending on the individual’s goals.
After the ingestion of creatine in foods or a supplement, it is absorbed in the gastrointestinal tract. Because of the structural similarity to amino acids, it has been hypothesized that it can cross the intestinal wall through amino acid or peptide transporters [8]. However, the presence of specific creatine transporters in the intestine has also been reported [9]. After absorption, creatine enters the bloodstream and circulates freely, allowing it to be taken up by target issues. This is suggested by an initial rise in plasma creatine levels, with a peak at about an hour after ingestion, and a subsequent decrease [3]. This process can occur due to the involvement of two types of creatine transporters – CreaT1 and CreaT2, which are highly expressed in the target tissues. The first of them can be found in the skeletal muscle, brain, heart, kidney, and testes, whereas expression of the second is presumably limited to the testes [10]. The bioavailability of the most extensively studied form of the supplement, creatine monohydrate, is nearly 100%, which means that it is almost fully absorbed and can be used by target tissues or excreted in the urine. Therefore, the amount of creatine retained by the individual can be calculated as a difference between its intake and urinary excretion [11]. The bioavailability of creatine may be affected by several factors, including the form of the supplement, the presence of other nutrients, and the individual characteristics of the person taking the supplement.
When taken in the recommended dosages, creatine is usually regarded as safe. However, there has been continuous discussion regarding the supplementation's potential risks. The adverse effect that is most frequently mentioned is weight gain. It can first be attributed to water retention and then later to an increase in muscle mass, which is usually desired by athletes [3, 5]. Gastrointestinal issues like bloating, diarrhea, and nausea are yet another potential side effect of creatine usage. Although its increased occurrence has been anecdotally recorded, there is no solid proof for it [3]. Due to fluid redistribution and ensuing electrolyte imbalance, several researchers hypothesized that creatine could cause muscle cramps or dehydration; however, this hypothesis was not supported by clinical evidence [3, 12]. Finally, there have been some concerns raised about the potential for creatine supplementation to cause kidney damage, but extensive research on this issue denied these suspicions as well [13].
Creatine and mental health disorders
The prevalence of mental health disorders in Europe is constantly growing, reaching 13.9% of the total disease burden in 2015 [14]. The COVID-19 pandemic has further significantly increased the frequency of the problem. The overall effect of the pandemic has been linked with worsening psychiatric symptoms [15]. The mainstay of treatment for many years has remained drugs from the group of neurotransmitter reuptake inhibitors [16], however, scientists are searching for new chemical compounds helpful both in the prevention and treatment of mental disorders. They are also sought because of the ever-important phenomenon of drug-resistant depression and the negative impact of depression on overall health which translates into an even greater burden on the healthcare system [17].
To understand the potentially positive effects of creatine in the treatment of depressive behavior, it is necessary to understand the likely molecular mechanisms that may be responsible for it. The brain is a highly metabolically active organ, consuming up to 20% of the body's energy. Not surprisingly, this organ has a specific brain isoform of creatine kinase (BB-CK), which is involved in the metabolism of high-energy compounds in the Cr/PCr/ATP shuttle pathway. This suggests that creatine is involved in providing and maintaining normal energy levels in the central nervous system [18].
A series of animal studies have been conducted to provide insight into the brain processes involved in creatine metabolism [19]. By using the proton magnetic resonance spectroscopy (1H MRS) technique on depressed rats, it was shown that creatine and phosphocreatine levels were reduced in the medial prefrontal cortex (mPFC), amygdala complex, and hippocampus [20]. The population of depressed rats was obtained by using a single-prolonged stress (SPS) model. It is based on inducing trauma in rats through a series of successive actions. For two hours, the rodents are immobilized by strapping their limbs with surgical tape to a metal board. They are then immediately transferred to a plexiglass cylinder and forced to swim for 20 minutes. After that, for 15 minutes they are left to dry out and finally treated with vapor ether until they lose consciousness. This sequence induces post-traumatic stress disorder (PTSD) and depressive behavior in rats thanks to which they serve as animal models for research on behavioral disorders [21]. In another study, creatine administration to rats with depressive behaviors was shown to reduce symptoms of the disease - however, this was sex-dependent - a significant improvement was observed only in females [22]. Even before these studies, it was proven that creatine behaves as a neurotransmitter in the brains of rats. It is accumulated and released from the cortex in an action potential-dependent manner. The main role in this process is played by sodium cations which is consistent with the involvement of Na+-dependent creatine transporter SLC6A8 in the passage of this substance into the brain. Even more significantly, after blocking sodium channels with tetrodotoxin (TTX), the secretion of endogenous and exogenous creatine was abolished. On the contrary, when potassium channels were blocked by 4-aminopyridine (4-AP), creatine-mediated transmission was significantly enhanced [23]. In addition, it was found that the antidepressant effect of creatine in mice is inhibited by compounds that inhibit PKA, PKC, CAMK-II, and MEK1/2, protein kinases that are associated with depression development [24]. The same group of researchers then concluded that it is the intracellular Akt, mTOR, and GSK3 pathways that are responsible for creatine's positive effects on mental health by observing a disappearance of this effect when PI3K inhibitors or mTOR inhibitors were used in rats [25].
Among humans, the results of studies of the relationship between creatine concentration in the brain and the incidence of depression are similar to those conducted on animals. The lower its level in the mPFC, the greater the likelihood of depression and, if it occurs, the clinical symptoms worsen as the concentration further decreases [26]. Also, population-based research has demonstrated the association between the intake of dietary creatine and the risk of occurrence of depression. Consuming more than 0.7 grams of creatine per day reduces the risk of depressive disorders by as much as about 30% compared to consuming less than 0.26 grams [27]. Despite the poor passage of creatine itself across the blood-brain barrier, an increase in creatine concentration in the gray and white matter was observed in a study with oral supplementation of creatine monohydrate following both a single high dose, as well as four weeks of supplementation. Three months after the end of its supplementation, its concentrations returned to baseline values [28]. Studies were also conducted with other substances occurring in the same metabolic pathway. Using phosphorus 31 magnetic resonance spectroscopy and brain transverse relaxometry it was shown that supplementation with 1,600 mg per day of oral S-adenosyl-L-methionine, a precursor to creatine, increases phosphocreatine concentrations and decreases transverse relaxation time, which translates into more efficient functioning of brain structures and greater energetic activity, as elevated relaxation time indicates atrophy of a given structure. The above compound had already been known and used as an antidepressant since the 1990s, however, it was this study that explored the molecular mechanism and clarified its therapeutic nature. Here, too, large gender differences were observed - in women the treatment effect was significantly greater than in men [29]. Another study directly comparing creatine and guanidinoacetic acid (GAA) supplementation showed that it was GAA that significantly increased creatine levels in the brain more than creatine alone and could be used as a butter substitute [30]. This superiority probably occurs due to the easier transport of GAA into the central nervous system, not only by the specific transporter SLC6A8, which is also responsible for creatine transfer but additionally by others like SLC6A6, GAT2 and passive diffusion [31].
Having the results of many studies in vitro and on healthy people, a pilot study on people with mental health disorders was undertaken. In patients with unipolar depression, after four weeks of 3-5 g/day creatine monohydrate supplementation, scores as measured by the Hamilton Depression Rating Scale and Clinical Global Impression Scale improved significantly [32]. Patients with bipolar depression after six weeks of supplementation (6 grams of monohydrate per day) showed improvement in the verbal fluency test [33]. In this case, however, no differences were observed in other neuropsychological tests. The supportive role of creatine in the treatment of classic antidepressants like fluoxetine is also emphasized. It is worth noting that a significant part of these studies was conducted only on women. However, some papers deny the helpful effect of creatine in treating depression with SSRI drugs [19].
Depression is not the only psychiatric disorder being studied for the role of creatine and its deficiency in the central nervous system. It has been observed that creatine concentrations in the hippocampus and occipital white matter are also reduced in PTSD and generalized anxiety disorder (GAD) [34]. So far, there is a lack of large, randomized trials in a group of patients with these disorders undergoing creatine supplementation, but there are some case reports and preliminary studies in which this method has been used with good results in reducing anxiety symptoms with previous treatment resistance [18, 19].
There are many in vitro and animal model studies that describe in great detail the likely molecular mechanisms of creatine action in the central nervous system, how it crosses the blood-brain barrier, and its metabolism. Many of these have been produced using magnetic resonance imaging, which has made it possible to identify specific relevant parts of the brain associated with mental health disorders and deficits in creatine concentrations that translated into poorer brain bioenergetics [1].
There is ample reason to believe that creatine levels in the brain affect mental health, and supplementation with it or its derivatives may help treat depression and other mental disorders. Pilot studies with patients seem to unanimously show a therapeutic effect of creatine supplementation and a reduction in symptoms of affective disorders [19]. However, there are no clear guidelines, dosages, or specific indications in which the use of this substance - or its derivatives - would be effective. This is due to the paucity of data from large studies, with dozens currently in the registry of randomized trials. In the coming years, we should expect new reports and perhaps a large meta-analysis unequivocally indicating the effect of creatine which will allow it to be introduced into widespread use.
Creatine and stroke
Stroke - considered a condition with two subtypes - hemorrhagic stroke and cerebral infarction - was a third global, Level 3 cause of death and disability in 2019 with 12,2 million incidents and 101 million prevalent strokes worldwide. If the current trend continues, there will be almost twice as many incidents and deaths caused by stroke in 2050 [35]. For this reason, there is an urgent need to develop new methods of prophylaxis and treatment. Studies about creatine supplementation seem to be a rational direction of exploration because of the ability of the Cr/PCr/ATP system to maintain energy availability in cells [36].
Research suggests that the brain relies on exogenous creatine to a lesser extent than muscles. Therefore, there have been doubts about whether oral creatine supplementation will increase its levels in the brain [18]. Nevertheless, two studies performed on mice, mentioned in the following section indicate a positive effect of oral supplementation in reducing infarct volume in case of a stroke [37, 38].
The objective of a study conducted by Zhu et al. [38] was to investigate the effects of creatine on reperfusion and neuroprotection in a mouse model of stroke. The authors measured the infarct volume, concentrations of ATP and creatine in ischemic and nonischemic brain tissues, and signs of apoptosis [39]: cytochrome c release and caspase-3 activation in the infarct area. Despite the lack of exhaustive information on the dose of supplementation, the study results were very promising, as evidenced by a 56% reduction in the infarction volume compared to the control group. Analysis of ATP and creatine in ischemic and nonischemic areas of the brain indicated a significant reduction in creatine drop after ischemia, and an even greater reduction of ATP drop in such conditions - approx. 56,3%. Another result was the inhibition of cytochrome c release and downstream caspase-3 activation in creatine-fed mice assessed in Western Blot analysis [38]. Moreover, observations regarding the effect of creatine on caspase-3 activation seem to be confirmed by a more recent study, designed in a human model. In response to acute running exercise, in addition to a statistically significant reduction in the concentration of plasmatic caspase-3 following 7-days supplementation at the dose of 20 grams per day - typical loading phase dosage [3, 12], also a statistically significant increase in the concentration of antiapoptotic protein bcl-2 was noted [40]. The underlying mechanism of the creatine influence on concentrations of mentioned markers – direct or indirect - remains unclear.
In the second mouse model trial by Prass et al. [37] beyond changes in nervous tissue, investigators focused on the effect of creatine on cerebral vascular functions. Therefore, they assessed and observed improvement in the capability to vasodilate in middle cerebral arteries isolated from mice in response to acidosis (pH = 7). Such or even greater acidosis may occur locally in the area of ischemia, which in turn may imply a local effect of supplemented creatine. Examination of central blood flow and apparent diffusion coefficient in vivo using magnetic resonance imaging indicated faster recovery from ischemia in the creatine-treated group. Examination of changes in levels of Cr/PCr/ATP concentrations in nervous tissue did not show any differences between the groups. Additionally, the study indicated a dose-dependent effect of supplementation on reduction in infarct volume and the lack of effect of intravenous administration of creatine on this parameter after the occurrence of stroke. Interestingly, feeding with chow which contained 2% monohydrate creatine (purity of 98%) over 3 months, showed a 42% reduction in infarct volume compared to the control group. On the other hand, in trials where investigators used the same dose over 12 months, there was no difference between groups. Conducting further research on this relationship seems rational due to the impossibility of predicting strokes and the necessity of long-term prophylactic administration associated with this fact [37].
The next great step in investigating the potential positive effects of creatine in cases of acute ischemic brain injury was a randomized, double-blind, and crossover design study conducted by Turner et al. [41] in which the influence of said supplementation on the excitability of corticomotor neurons and cognitive performance under conditions of reduced oxygen supply was examined. Fifteen healthy, right-handed participants aged from 21 to 55 underwent 7-day supplementation at the dose of 20 g per day (loading phase dosage [3, 12]) with a 5-week washout period. After hypoxia intervention, which was inhalation of a 10% oxygen gas mixture for 90 min via face mask system with a valve, neuropsychological assessment, neurophysiological and neuroimaging procedures among others were performed. Results of magnetic resonance spectroscopy confirmed that oral supplementation can increase the concentration of creatine and phosphocreatine in the sensorimotor cortex. Results of several neuropsychological tests showed that creatine supplementation has a positive effect on performing tasks involving complex attention during hypoxia. Assessment based on stimulus-response curves of the first dorsal interosseous muscle motor cortex showed that creatine supplementation increases corticomotor excitability during hypoxia compared to the control group [41].
Research on novel derivatives of creatine is an important and exciting area in the context of preventive supplementation. The goal is to create a medication for situations where the creatine transporter is impaired and conventional creatine supplementation is insufficient [42]. One of the key parameters being studied is the ability to increase Cr/PCr/ATP concentrations in nervous tissue [43], which could significantly impact creatine's role as an energy buffer in the brain. Additionally, better BBB penetration could allow for more optimal dosing, where higher concentrations could be achieved in the central nervous system while reducing the dose, which may be crucial for patients at risk of accompanying diseases who are undergoing supplementation.
Another significant problem associated with stroke is its consequences. Patients who have suffered from this condition may experience decreased strength and endurance, sarcopenia [44], as well as psychological symptoms, including anxiety, depression, or PTSD [45]. Therefore, this group of patients requires special care and rehabilitation to improve their daily functioning and quality of life [46]. For this reason, Butchart et al. [47] investigated the effect of creatine supplementation added to progressive resistant training (PRT) in a population of stroke survivors on different aspects affected by stroke, such as body composition, exercise capacity, or levels of anxiety. The study revealed PRT itself had a positive impact on muscles, namely their strength, and thickness. Moreover, it improved patients’ balance, and cognition and decreased levels of depression. Added creatine further increased the benefits by improving walking performance, enabling the patients to cover longer distances in a 6-minute walk test. Therefore, creatine supplementation might be useful not only in the prevention of stroke but also in the treatment of its consequences.
In the case of stroke, the studies presented above regarding the prophylactic effects of creatine, despite many promising results, are not able to provide definitive evidence for the beneficial effects of creatine supplementation in this population of patients [37, 38]. However, they are a good basis for designing larger studies on the long-term use of creatine in at-risk groups, which could bring us closer to understanding the real effects of such a procedure in stroke cases and at the same time dispel any doubts regarding the differences in the effects of long- and short-term creatine supplementation on the course of cerebral ischemia [37]. It is also important to keep an eye on ongoing research on new derivatives of creatine [43, 48], which may provide new data on the protective effect of this compound in the case of cerebral ischemia or even change the current perception of such a procedure.
An additional important point of research into the use of creatine in diseases related to the central nervous system will be to grapple with the poor permeation of creatine across the blood-brain barrier [49]. The development of new substances or the possibility of better penetration of monohydrate into the brain will allow for more rational dosing and a reduction in possible adverse effects of the therapy [30].
Creatine and heart failure
Heart failure (HF) is one of the serious health burdens of our times affecting over 60 million people around the globe [50]. According to a definition proposed in the consensus statement of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society, and Writing Committee of the Universal Definition of Heart Failure, HF is characterized by structural and/or functional cardiac dysfunction corroborated by elevated natriuretic peptides in association with pulmonary or systemic congestion. Even though HF is a heterogeneous syndrome complex with complicated etiology and it is being escalated by a wide range of comorbidities, scientific bodies distinguish hypertension and ischemic heart disease as main cofactors in the development of HF [51].
To maintain its valid function, the heart needs a continuous production of ATP [51]. It is strictly linked to the fact that the amount of ATP that the human heart uses every day adds up to 6000 grams of this compound, which is approximately 20 times its weight. Without its constant production, the heart would deplete the immediate ATP reserves within 2-10 seconds, leading to functional impairment [51, 52]. Therefore, it is clear that if the heart is not able to store ATP, the process of its production has to be very effective and perfectly organized. The machinery of maintaining proper ATP levels has 3 main branches. Firstly, substrate utilization, secondly mitochondrial respiratory chain and finally energy-transfer mechanism termed the creatine kinase energy shuttle [52]. Maintaining a proper level of ATP in heart cells is crucial for keeping the proper function of cardiomyocytes [51].
In a cardiomyocyte of a failing heart, the ATP supply is lower than ATP demand which derives mainly from altered cardiac metabolism and unfavorable geometry caused by remodeling [53]. Yet there are several mechanisms that cardiomyocytes use to protect themselves from negative results of this state and one of them is the creatine phosphate energy shuttle with a mechanism of providing ATP by CK. Multiple studies suggest that particularly this metabolic function is impaired in HF and is one of the important factors that contribute to the progression of this condition [54, 55].
The fact that the total pool of ATP, and phosphocreatine are decreased not only in animal models with induced HF but also in humans with a failing heart, has been known for many years now [56]. More recent studies with the use of magnetic resonance spectroscopy instead of biopsy tend to clarify and confirm those results [57, 58]. Apart from levels of those markers, another useful indicator of the myocardial metabolic state is the PCr/ATP ratio. As expected, several studies confirm the thesis that the PCr/ATP ratio is diminished in patients with HF [59, 60]. It could suggest that the mentioned indicators (PCr/ATP ratio, [PCr], [Cr]) could be good predictors of HF progression. Indeed, Samuel et al. [61] showed a correlation between decreased ATP levels in cardiomyocytes and a higher risk of life-threatening arrhythmias. Bottomley et al. [62] report that the ability to synthesize ATP through creatine kinase (CK) is a predictor of HF as well as mortality (both overall and specifically from cardiovascular causes). However, those indicators lack specificity as they can also be diminished in comorbidities such as diabetes type 2 [63]. The next problem is the clinical significance of those markers including practical use since imaging the phosphorus content of a failing heart requires suitable equipment, and technicians, and absorbs financial resources [62].
An interesting study that has been conducted by Ten-Hove et al. [64] showed a significant role of creatine during stress in rodents’ hearts. Mice without the enzyme which allows them to synthesize creatine - guanidinoacetate-N-methyltransferase (GAMT), were stimulated by dobutamine and underwent ischemic conditions. At baseline, without stressful stimulation, GAMT-knocked out mice and normal mice did not differ in terms of diastolic and systolic function. Nevertheless, after initiation of a stressful situation (ischemia/reperfusion and inotropic stimulation), mice without the ability to use ATP-creatine shuttle had impaired cardiac inotropic reserve and worse recovery of contractile function after reperfusion [64]. Similar conclusions were drawn by Lygate et al. [65] who created a group of mice with higher concentrations of intramyocardial creatine levels. This state was developed by modification of creatine transporter (CrT) in the heart of rodents. Mice with modified CrT had better results in ischemia/reperfusion situations while no significant difference in the development of chronic HF was observed. This study might suggest that the role of the Cr/PCr/ATP shuttle is most important in short-term energy intake increase, such as during ischemia or elevated energy demand which are situations naturally occurring in the course of HF [52]. Similar studies conducted by various researchers based on taking out the function of creatine shuttle showed analogous results confirming the thesis above [66, 67].
As evidenced above, HF is very closely linked with heart metabolic dysfunction including impairment of the Cr/PCr/ATP shuttle and CK flux. Therefore, is it possible to fix those impairments through creatine supplementation and improve the function of the heart along with the level of physical performance in patients with chronic HF? As much as this approach seems reasonable, taking into consideration the basic pathophysiology of HF and the mechanisms described above, the available studies on this topic do not unanimously support this idea and list several problems.
The first problem with the way to use creatine supplementation as an add-on therapy in HF is that some studies report that increasing intramyocardial levels of creatine is not as simple as it seems. Several researchers suggest that this issue may be the result of down-regulation of the creatine transporter which occurs in the plasma membrane as well as the mitochondrial membrane. Levels of this protein are strictly linked with intracellular levels of creatine and could be a limiting factor [65].
Furthermore, a study conducted by Boehm et al. [68] suggests that increased intake is ineffective in raising myocardial creatine levels in rats. In tune with that, Lygate et al. [65] while investigating the protective influence of myocardial creatine levels in HF and ischemia in mice, increased myocardial creatine levels by upregulating CrT expression and not by oral supplementation. According to those studies, creatine transporter also seems to be a significant factor in developing HF, and determining intracellular levels of creatine, can complicate the therapeutic use of this supplement. However, it could also be a potential aim for drug research that could be used in patients with chronic HF in the future [69]. Further investigation performed on animal models with infarction caused by artery ligation revealed that raised creatine levels in myocardial cells did not prove to be protective in terms of developing hypertrophy, dilation as well as impaired function of the left ventricle. On the other hand, they give optimistic results in ischemic reperfusion models where mice that underwent creatine supplementation were almost as resistant to these damages as models with ischemic preconditioning [65, 70]. Similar results were obtained in a study where researchers added ribose supplementation to elevated levels of myocardial creatine in experimental mice with overexpression of CrT [71]. D-ribose is a diet supplement that directly increases the production of phosphoribosyl pyrophosphate and ATP in the myocardium. This provides the protective function of this compound in situations when ischemic stress occurs [72]. However, the treatment used in this study did not prove beneficial in the prevention of developing LV dysfunction and remodeling in experimental mice that suffer from chronic myocardial infarction. Taking into consideration studies where the elevation of not solely creatine levels in the myocardium but also increased expression of CK was applied, an interesting study was conducted by Gupta. Mice with those modifications (overexpression of CK and increased creatine myocardial level) stood out with better systolic function, cardiac output, and improved survival. Worth mentioning is the fact that remodeling again has not been positively affected and improved function of the heart required constant overexpression of CK [73].
Analyzing trials conducted clinically, discrepancies in study constructions and results are apparent. The varying designs of those studies including different doses, length of observation, and additional substances that are being analyzed together, make it very hard to clearly express the significance of those results. Despite this fact, we tried to gather all relevant studies conducted on this topic and tried to answer the question of whether the use of creatine or further research in this field is reasonable.
One of the biggest studies taking up the topic of creatine supplementation and HF was one conducted by Cornellisen et al. [74] which aimed to investigate the positive influence of creatine supplementation as an add-on to aerobic exercise and tried to compare it to patients who underwent physical exercise but did not use creatine supplementation. The study was well designed with sample size exceeding those observed in other quoted studies. Physical endurance and peak VO2 were increased in all patients undergoing physical therapy but no differences between the placebo and creatine groups were observed in any of the measured endpoints. Fumagalli et al. [75] using a population of over sixty patients conducted a double-blind randomized study that proved a statistically significant benefit in life quality and exercise tolerance from supplementation of creatine combined with coenzyme q10 (CoQ10) (doses 340 mg and 320 mg respectively) for 2 months. Exercise tolerance was measured by cardiopulmonary exercise test (6MWT and VO2) so those values could be considered as accurate predictors of patients’ ability to perform daily activities. Worth noticing is the level of the creatine dose, which was relatively low compared to standard supplementation doses, as well as the simultaneous use of CoQ10, both of which may suggest that the positive effect was obtained mainly by the use of CoQ10. However, studies analyzing the impact of CoQ10 on exercise capacity also show a certain level of discrepancy making it even harder to answer which of the supplements was responsible for obtained results. Effect of the creatine supplementation on physical performance (measured also by peak VO2 and 6MWT), life quality, and ejection fraction were examined by Kuethe et al. The study was conducted on a small population (20 patients, 7 of which lost to follow-up) in a double-blind crossover manner. In contrast to the previously described study, this one did not show a significant difference between the placebo and experimental groups in physical performance or intensification of dyspnea in the Borg scale. Nonetheless, muscle strength and body weight were increased which seems understandable due to the osmotic effects of the supplemented compound. Similarly, a study conducted by Carvalho et al. did not prove that creatine supplementation increases the performance in any of the investigated endpoints (6MWT, peak VO2, or perceived extortion measured by the Borg scale) [76]. However, the sample size of both studies was low and in addition, in a trial conducted by Carvalho et al. [76], only males were recognized as eligible. These facts remarkably decrease the reliability of presented studies and the expected small differences resulting from creatine supplementation could be easily overlooked.
Apart from studies analyzing the influence of creatine supplementation on aerobic capacity and endurance in patients with cardiovascular (CV) impairments, some researchers tried to determine the correlation of this intervention with certain muscle groups' endurance and strength in patients with these diseases. Andrews [77] tried to investigate the effect of creatine supplementation on muscle endurance in patients with HF using a forearm hand grip dynamometer. This study revealed an increase in exercise tolerance and metabolic response to physical exercise in a group of males with HF. However, it is important to determine the clinical significance of such an upswing in this subgroup and eventually confirm those results in a larger study. The dose of creatine in this study in contrast to Fumagalli was higher than standard doses of monohydrate (which is 5g administered orally) but the duration of supplementation raises some doubts about the effectiveness of such a course of supplementation (study conducted only for 5 days with 20 grams of creatine daily) [77]. Gordon et al. [78] tried to determine the effect of high-dosage creatine supplementation on muscle endurance and strength determined by the use of knee extensors as well as on ejection fraction in patients with HF. The study did not show significant differences in physical endurance between the experimental group and placebo before and after supplementation, similar to the EF measures which also did not differ, in opposition to researchers’ expectations from previously analyzed studies. Interestingly, the increase of the creatine levels in skeletal muscle measured in this study was significantly greater in patients with low baseline levels of creatine content in skeletal muscles. This could suggest that this group is especially prone to react positively to creatine supplementation and should be targeted during such adjuvant treatment aiming to increase extortion tolerance and strength in those patients. However, the reliability of this study is highly questionable taking into consideration aspects of sample size, and evaluating the effects of blinding [78].
To conclude, all data presented above, despite traces that could suggest that creatine supplementation could improve cardiac function in HF, suggests that it mainly affects muscle strength, while physical endurance seems to be unaltered. Theoretically speaking, creatine could prove beneficial in increasing endurance and quality of life in patients with HF but at this moment there is a lack of any strong evidence to support this hypothesis.
Creatine and vascular health
The ergogenic role of creatine has been studied neatly in recent years and the use of this most popular sports supplement is gaining popularity in various groups of receivers in many fields of sport and medical research [3]. However, apart from the mechanism of creatine action which comprises the Cr/PCr/ATP chain and energy buffer system, several other mechanisms of action are postulated, including help in the management of oxidative stress [79]. Studies conducted in past years allow us to suspect creatine as a potential antioxidizing agent which opens more than a few possibilities of the potential use of this supplement in various diseases, including those concerning CV issues [80].
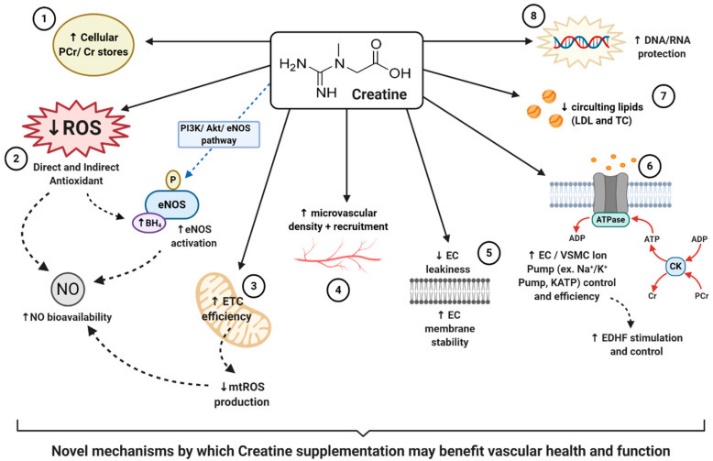
Most CV disorders are paired with worsened vascular function. In many cases, it goes along with disrupted synthesis and attenuation of ROS which results in the accumulation of those compounds and the development of vascular disorders. There are several ways in which creatine may support vascular health [81]. Hypotheses explaining this potential benefit are shown in (Figure 2).
|
|
|
Figure 2. Novel mechanisms by which creatine supplementation may benefit vascular health and function; PCr = phosphocreatine, Cr = creatine, EC = endothelial cell, DNA = deoxyribonucleic acid, RNA = ribonucleic acid, ETC = mitochondria electron transport chain, mtROS = mitochondrial-specific reactive oxygen species, ROS = reactive oxygen species, LDL = low-density lipoprotein, TC = total cholesterol, PI3K/Akt/eNOS pathway = Phosphatidylinositol 3-kinase/Protein kinase B/endothelial nitric oxide synthase pathway, eNOS = endothelial nitric oxide synthase, P = phosphorylation, BH4 = tetrahydrobiopterin, NO = nitric oxide, ADP = adenosine diphosphate, ATP = adenosine triphosphate, CK = creatine kinase, VSMC = vascular smooth muscle cell, Na+/K+ Pump = sodium/potassium pump, KATP = ATP-sensitive potassium pump, EDHF = endothelium-derived hyperpolarization factor, ↓ = decrease/reduction in, ↑ = increase in, image from Clarke et al. [81] |
Therefore, the use of creatine supplementation for prevention or to help in recovery and improve the daily functioning of patients with CV disease seems a logical approach. Undoubtedly, this topic is very poorly studied and none of the listed papers concentrates specifically on CV patients and tries to approach the topic taking into consideration the clinical significance of such intervention.
Moraes et al. [82] in an open-label study tried to determine the influence of oral creatine supplementation on systemic microcirculation and homocysteine levels. The study was conducted in a group of young healthy individuals. The experimental group after the course of 1-week creatine supplementation had increased basal capillary density measured in capillaroscopy. Considering that several retrospective studies determined decreased capillary density as a hallmark of hypertension and that some of those studies suggest that capillary density rises when this disease is treated properly, it can be concluded that arterial blood pressure (BP) could be strictly connected with capillary rarefaction [83, 84]. What is interesting, significant differences were also observed in mean BP which was lower in the creatine group, with no differences separately observed in systolic and diastolic BP. Despite the statistical significance of this finding, the clinical relevance remains questionable (92.1 ± 1.1 vs. 89.8 ± 1.1 mmHg, P = 0.0255). Also, regarding the fact that all BP values were measured in normotensive healthy males, the ability of creatine to decrease BP is doubtful but surely needs further investigation. On the other hand, significantly decreased levels of total [174.0 (143.5-204.0) vs. 174.0 (140.0-197.5) mg/dL, p = 0.0486] and LDL-cholesterol [115.0 (88.0-142.5) vs. 103.0 (81.0-130.0), P = 0.0027] are promising results which can suggest that creatine could play some role in maintaining proper cholesterol levels which is an essential risk factor in many CV diseases [85]. Homocysteine levels were not altered after creatine supplementation, contrary to what authors expected, and previous studies have shown [86, 87]. However, an increased level of plasma creatinine was observed.
Likewise, in a study by Van Bavel et al. [88] after 3 weeks of regular creatine supplementation, a significant increase in basal capillary density was observed. Worth mentioning is the fact that this study was conducted in a group of people following strict vegetarian diets. The level of creatine in people undergoing this type of diet was initially depleted which can suggest that this effect could be only visible in a population with primary decreased levels of this compound. In contrast to the study conducted by Moraes et al. [82], levels of homocysteine differed significantly between the groups - they decreased in the experimental group compared to the placebo.
Arciero et al. [89] tried to determine the effect of creatine supplementation combined with resistance training on indicators such as body composition, muscular strength, and limb blood flow. Similarly, a study by Moraes et al. [82], was conducted on a group of healthy males in a double-blind randomized manner. The study has shown that the addition of creatine as an add-on to standard resistance training increases levels of fat-free mass as well as calf and forearm blood flow (peripheral blood flow). Results also suggest that an increase in metabolic rate could be obtained by creatine supplementation alone, regardless of performing resistance training. In agreement with the study conducted by Moraes et. al, the study reports that cholesterol blood levels were decreased significantly in the group with creatine added on to resistance training (172 ± 27 vs. 155 ± 26 mg/dL, P < 0.01) in opposition to the group with placebo (162 ± 32 vs. 161 ± 36 mg/dL). Also, as expected, muscle strength was increased in all groups in tune with loads of data presented in previous years, in multiple studies. Those results are promising and may suggest using creatine as an add-on, for example, in rehabilitation courses where physical training is routine or for patients who perform daily physical activity. But this study unfortunately does not deliver data suggesting that creatine alone has an influence on blood flow and vascular function and for sure more developed randomized trials with a bigger number of participants are obligatory to determine this issue.
A study performed by Sanchez-Gonzales et al. [90] sought to establish whether creatine supplementation has a positive influence on vascular responses after performing an isokinetic exercise. Healthy males with a median age of 22 were found eligible for this study (16 volunteers in total). The study has shown results suggesting that the use of creatine as a daily supplement attenuates the escalation of heart rate and systolic BP after isokinetic exercise. De-escalation of these parameters, according to multiple studies, could prolong patients’ life, and prevent or slow down the progression of disease if only those parameters were also under control at rest. However, there were no changes observed in any of the measured parameters before performing the physical exercise. What is more, the study was performed on healthy young males so it can be expected that the response of patients with CV diseases could be entirely different. Further research is needed to determine the mechanism of those actions as well as the clinical application that can be obtained from those results.
Cr/PCr/ATP plays a major role in cardiac metabolism especially when it comes to situations when energy supply is depleted or impaired [91]. That’s why the thesis that cardiac metabolism as well as the owner of a stated heart could profit from creatine supplementation, seems reasonable. Yet, gathered and analyzed studies do not unanimously support this thesis. It must be stated that currently, there is a lack of direct evidence that creatine could be a useful supplement in any CV disease. On the other hand, a noteworthy fact is that some studies demonstrated that the CV system could benefit in different ways from regular supplementation of creatine [75, 82, 89]. However, all of them have been conducted on healthy volunteers, therefore the presented data is definitively too weak to support the use of this supplement regularly in CV patients. Nonetheless, the enticement to search for trustworthy evidence supporting the confronted thesis is large as creatine is a ubiquitous supplement that is relatively cheap and stripped of side effects compared to drugs commonly used in cardiology.
Particularly interesting is the effect of creatine on the performance of patients with CV disease which was examined in several studies presented in this paper. None of them showed a significant benefit from adding creatine to the diet of those patients which stays in opposition to studies on creatine in healthy athletes [74, 76]. Nevertheless, the presented vision is encouraging and a large, valid randomized study, which would investigate the intricacies of increasing performance in CV patients could disperse any ambiguities.
Undoubtedly, creatine is experiencing its golden times as exhaustive research regarding this substance, with tons of evidence supporting its use in sports, has made it one of the most commonly used supplements in the world [1]. Its pivotal role in energy metabolism has led to the emergence of many ideas considering the use of this compound in different health issues. Recent years have resulted in a huge number of studies investigating these non-sport applications, however, some imperfections in study designs or small sample sizes make it challenging to draw strong conclusions from them.
Looking at creatine supplementation from a practical point of view, it has some significant advantages as well as disadvantages. First, creatine is a relatively cheap and widely available supplement with a good safety profile when taken in recommended dosages [3, 5]. Moreover, it is available in many forms, ranging from pills, and powders, to beverages, therefore potential recipients can choose the formulation that is most convenient for them [8, 12]. However, it has also some drawbacks. There is a population of patients considered non-responders, with limited ability to uptake creatine, so the benefit observed in them might be less visible [92]. Moreover, one of the frequently reported side effects is water retention, which is highly undesirable in CV patients, who often present with edema [5]. Finally, since creatine levels return to the baseline 4-6 weeks after stopping the supplementation, for long-term results it has to be taken consistently over a longer period [3].
The health problems cited above are not the only ones in which the potential role of creatine is being investigated. In most of the following examples, there is a lot of controversy and ambiguity in the results. Effects on other diseases of the nervous and neuromuscular systems - Huntington's disease and Parkinson's disease - have been studied. Despite promising data from the initial papers, later placebo-controlled randomized pilot trials failed to show any improvement in the state of patients - in both of the conditions [93, 94]. Similar results were obtained for amyotrophic lateral sclerosis (ALS) [95]. However, in the case of muscular dystrophy diseases, a meta-analysis conducted by the Cochrane Library proved improvements in both muscle strength and overall function with creatine supplementation with good tolerance of the drug and no reported clinically relevant adverse events [96].
Another field of medicine where the potential of creatine could be used is geriatrics. Common conditions which often accompany people in older age include osteoporosis, sarcopenia, or cachexia. In all of these indications, creatine has been investigated as an adjunctive treatment. Research shows that supplementation, especially in conjunction with resistance training, has the potential to reduce the negative impact of aging on muscles [97]. Notably, creatine was shown to improve sit-to-stand performance in older adults, which has great clinical significance, since it is a predictor of reduced risk of falls [98, 99]. Nevertheless, the results of studies investigating the effect of creatine on bone health are unambiguous [97, 100]. Since bone is a tissue that has a long remodeling cycle, large trials investigating the long-term effect of creatine supplementation on bones are required to establish its role in supporting patients with osteoporosis [97].
CONCLUSION
Taking into consideration the functioning of the Cr/PCr/ATP shuttle as well as the pathophysiology of diseases mentioned in this review, creatine supplementation in these conditions seems rational and justified. However, a huge number of studies that have been performed in recent years have come up with unambiguous results. Moreover, inconsistency, imperfections in study designs, or small sample sizes make it challenging to draw strong conclusions from these trials. That is why future direction in research in this field should carefully cover these areas. The coming years will show whether the hope placed in creatine supplementation as an adjunctive treatment in the mentioned conditions was valid or in vain.
ACKNOWLEDGMENTS: The authors are highly grateful to the staff of the Department of Pharmacology, Jagiellonian University Medical College, for their guidance and support during the research.
CONFLICT OF INTEREST: None
FINANCIAL SUPPORT: None
ETHICS STATEMENT: None